
Philip R. Liebson
Chicago, Illinois, United States
“I do not imagine that electrocardiography is likely to find very extensive use in the hospital . . . It can at most be of rare and occasional use to afford a record of some anomaly of cardiac action.”
—Augustus D. Waller, 1911
Perhaps the earliest technical device that was to become the electrocardiograph (ECG) was developed in 1820. In that year the Danish scientist Christian Oersted measured the changes in electric current by the deflection of a needle, named a galvanometer after Alysio Galvani, who in 1790 used electrical stimulation to move a frog’s legs. The next step came in 1842 when the mathematician Carlo Matteucci introduced the term “action potential” by isolating a nerve from a frog limb, stimulating the nerve, and causing the underlying muscle to contract.
This achievement was followed in 1868 by Julius Berstein’s use of a rheotome to measure the time course of electrical activity in muscles. Within a year Alexander Muirhead, at St. Bartholomew’s Hospital in London, successfully recorded the electrical activity of the human heart using a siphon used to record transatlantic signals.
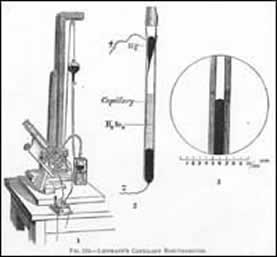
Over the next few decades there was considerable progress in the measurement of cardiac electrical activity. Four years after Muirhead’s application, Gabriel Lippman created a capillary electrometer. This device was composed of a glass tube containing mercury, one end of which was drawn out as a capillary tubing immersed in a bath of sulfuric acid. The sulfuric acid caused the mercury meniscus to move with changes in the electrical potentials in the bath, projecting an image on a screen. This image was then recorded on photosensitized paper. For this work, he received the Nobel Prize in physics in 1908.
It was in 1887 that the first human electrocardiogram was performed, with use of the capillary electrometer, by Augustus D. Waller, a physician and physiologist. First called an electrogram, its name was changed to cardiogram. Recordings were made from the chest wall and from the esophagus. He noted the two prominent deflections, the QRS and T waves which he called V1 and V2 respectively. In 1911, three years after Lippman received the Nobel Prize for his work, and after Einthoven’s early studies, Waller stated, “I do not imagine that electrocardiography is likely to find very extensive use in the hospital. . . . It can at most be of rare and occasional use to afford a record of some anomaly of cardiac action.”
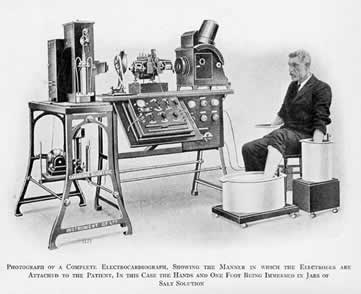
By 1901 Willem Einthoven (1860-1927) had completed work on the string galvanometer. String galvanometers had been used to amplify signals across long-distance submarine cables but his device was much more sensitive. The device consisted of a very thin filament of conductive wire passing between very strong electromagnets. When a current passed through the filament, the string moved because of the change in the electromagnetic field. The electrical activity of the heart was recorded on photographic paper from a light passing through the string. The early machine needed water for cooling because of the electromagnetic field, required 5 people to operate, and weighed 600 pounds. In addition, the patient was required to keep a leg and an arm in a bucket of water.
Willem Einthoven, born in Samarang, Java of Dutch and Swiss parentage, was taken to Utrecht, Netherlands by his mother when his father, a doctor, died when Willem was 6 years of age. He received a medical degree at Utrecht in 1885 and became a professor in Leiden the following year, unusual for such a young physician, but fortuitous because of the death of the incumbent professor and the influence of a distinguished ophthalmologist and professor at the university. In 1903 he developed the first practical ECG and in 1924 he received the Nobel Prize for the discovery of the mechanism of the ECG. He also invented the terminology P, QRS, and T for the deflections in 1895. The term “Einthoven’s Triangle,” the imaginary equilateral triangle centered in the chest and indicating the orientation of the standard limb leads, was named for him.
Einthoven first published his recordings in 1902. It is interesting that in 1897, a French engineer, Clément Adler had produced a similar instrument for use in communication, which Einthoven acknowledged in a paper the previous year. After developing an expertise in differential and integral calculus, he published several papers in the mid-1890s demonstrating the use of differential equations to correct the poor bandwidth tracings from the capillary electrometer. These calculations could be used to approximate the true form of an ECG that would have been recorded without the limitations of the frequency response. The string galvanometer had a high sensitivity that did not require the mathematical corrections needed for accurate recordings taken with the capillary electrometer.
By 1909 he had published his first detailed description of his string galvanometer and other papers that detailed descriptions of various ECGs from patients with cardiac abnormalities. Over the next few years, the string galvanometer became a fixture in physiology laboratories throughout the world and in most hospitals. The simplified electrocardiographic apparatus was developed and pioneers in electrocardiography, such as Sir Thomas Lewis , used the ECG to diagnose and classify dysrhythmias and pattern of abnormalities in cardiac conditions. But that is another story.
Einthoven died in 1927. He never recorded his own electrocardiogram.
References
- Katz LN, Hellerstein HK. Electrocardiography pp 255-351, in Circulation of the Blood. Men and Ideas. Alfred P. Fishman and Dickinson W. Richards Eds. American Physiological Society, Bethesda MD 1982.
- Rivera-Ruiz M,Cajavilca C, Varon J. Einthoven’s string galvanometer. The first electrocardiograph. Tex Heart J 2008; 35: 174-178.
- Kligfield P. Derivation of the correct waveform of the human electrocardiogram by Willem Einthoven, 1890-1895. Cardiology J. 2010;17:109-113.
PHILIP LIEBSON, MD, graduated from Columbia University and the State University of New York Downstate Medical Center. He received his cardiology training at Bellevue Hospital, New York and the New York Hospital Cornell Medical Center, where he also served as faculty for several years. A professor of medicine and preventive medicine, he has been on the faculty of Rush Medical College and Rush University Medical Center since 1972 and holds the McMullan-Eybel Chair of Excellence in Clinical Cardiology.
Highlighted in Frontispiece Volume 5, Issue 2 – Spring 2013