
Göran Wettrell
Sweden
The developments in ultrasound and microwave technology during World War II stimulated further research in the early 1950s. Ultrasound had been predicted to be useful in visualizing the organs of the human body, and with the beginnings of cardiac surgery there arose a need for better preoperative diagnosis, especially for correcting mitral stenosis in adults.
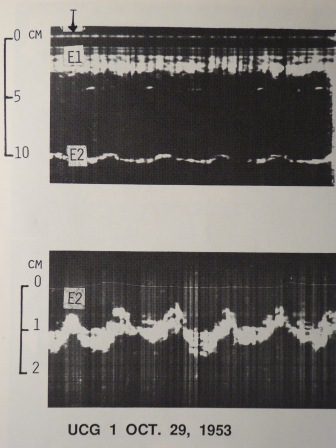
At the University of Lund in Sweden, early cooperation between clinical medicine and technology developed the ultrasoundcardiogram. Translational biomedical-technical research and teamwork led to the first ultrasoundcardiogram/echocardiogram being recorded on October 29, 1953, (Figure 1) as a result of the collaboration between the cardiologist Inge Edler and the physicist Hellmuth Hertz (Figure 2).
Chance favors the prepared mind
In Europe, early ultrasound research focused on clinical problems whereas in America studies were more theoretical. In May 1953, Inge Edler and Hellmuth Hertz met to discuss the possible use of ultrasound for cardiac investigations. Edler’s aim was to evaluate patients with mitral stenosis—sometimes combined with mitral insufficiency. The surgical procedure at the time was forced dilatation of the mitral valve (closed commissurotomy) and if the patient also had mitral insufficiency he would not improve. How then could ultrasound be used to estimate volume changes of the heart and especially of the left atrium?
Hellmuth Hertz, being well acquainted with the ultrasonic reflectoscope for material testing, suggested that this instrument might also be useful to measure left atrial enlargement. He also knew that such an instrument happened to be available at a shipyard in a nearby town where it was used for testing materials. On a weekend in May 1953 they borrowed the reflectoscope and studied several patients. They saw a moving echo signal in a patient with mitral disease at a depth of about 10 cm from the transducer applied on the anterior chest wall; and the echo was supposed to come from the posterior wall of the heart. Hertz then found out that the Siemens Corporation in Germany was building ultrasonic reflectoscopes for industrial use. His father, Gustav Hertz, the Nobel Prize winner in Physics of 1925, had been a director of Siemens Research Laboratory and thus his son Hellmuth was able to contact the Siemens medical branch in Erlangen and to demonstrate the preliminary findings of their heart investigations. A reflectoscope was immediately sent to Lund for a loan for one year: it was never returned (Figure 2).

The reflectoscope arrived in Lund on October 1953. The first experiments were designed to show that the blood/heart wall interface reflected ultrasound and could be recorded. The optimal ultrasound frequency used in adults was 2.5 MHz produced by a 12 mm flat quartz crystal. The experiments included transected isolated human heart preparations, and it was possible to localize interfaces between the heart and blood-filled cavities as well as an echo signal from a needle placed in the chambers as well as an auricular thrombosis. In patients with aortic regurgitation it was possible to show an impressive amplitude of systolic movement and also the thickness of the posterior heart wall. After a few weeks training, echoes from the anterior mitral leaflet were recorded in patients with mitral valve disease. However, the echo at first was supposed to originate from the anterior part of the left atrium, close to the mitral annulus.1
The visual observation of the echo-signal on the oscilloscope screen (A-mode) gave information chiefly about distance. Continuous recording of this motion was required. Therefore Hertz built a camera with film at a constant speed placed in front of the oscilloscope. Thus the photographic M-mode recorder with simultaneous recording of ECG was developed. The results of the first investigation on patients were published in March 1954 with the title: “The use of ultrasonic reflectoscope for continuous recording of the movements of heart walls.” 2
Further developments in Lund of ultrasound of the heart
At first most of the scientific work in Lund was devoted to movements of the mitral valve, but a pericardial effusion was diagnosed by ultrasound in 1955 and an atrial myxoma a year later.4 In 1961 in a thesis titled Ultrasoundcardiography, Edler summarized his findings, describing ultrasound as a diagnostic aid to evaluate biological tissues, mitral and aortic valve movements, and atrioventricular valve motility in living humans.3 He also attempted a transoesophageal investigation, but without success.
Interest in this new method in Scandinavia was astonishingly low. In Sweden funding for further scientific work was refused, and interest in further research now moved to other countries such as the United States and the Netherlands. In 1963 Harvey Feigenbaum in Indianapolis began to use ultrasound for investigating pericardial effusions. He organized the first course in the use of ultrasound/echocardiography in 1968, and Dr. Inge Edler was in the audience.
Hertz continued the technical development to create two-dimensional cross-sectional images of the heart. Already in 1960 the first mechanical instrument had been built in Lund. The technique was further developed, leading to the use of a mirror system and the first real-time cardiac ultrasound scanner in 1967, further improved by increased frame-rate in 1972.1,4 Hertz also developed and modified an ink-jet recorder for continuous M-mode curves, made even in color.5
In the early 1960s Inge Edler and Kjell Lindström (the latter a co-worker of Hertz) attempted to measure intracardiac blood flow with Doppler equipment. They carried out tests first on isolated heart preparations and then on patients, and were able to report on clinical Doppler measurements of leakage in the aortic and mitral valve at the first World Congress on Ultrasonic Diagnostics in Medicine in Vienna in 1969.4
By the mid 1960s, Dr. Nils-Rune Lundström had established a unit of pediatric cardiology in Lund. At that time the diagnosis was based on physical examination, ECG, and cardiac catheterization, but when after a few years two young patients appeared with suspected mitral valve disease, Dr. Inge Edler was contacted and demonstrated the usefulness of ultrasound by diagnosing mitral stenosis in one patient and cor triatriatum in the other. Thus began the use of ultrasound in pediatric patients with congenital heart defects and in establishing normal pediatric ultrasound values for intracardiac dimensions. The experiences of Dr. Lundström were presented at the First World Congress of Ultrasonic Diagnostics in Medicine in Vienna in 19694 and included showing findings in Ebstein’s anomaly of the tricuspid valve, congenital mitral stenosis, cor triatriatum, hypoplastic left heart syndrome, and membranous subaortic stenosis. There was at that time only one published article of preliminary observations on a young patient with membranous subaortic stenosis.4 With the available technical equipment, a diagnostic echocardiographic investigation of pediatric patients required an advanced skill which took much hard work to achieve. In 1972 and 1973 Dr. Lundström published three articles in Circulation on the diagnosis of specific cardiac malformations by ultrasound.6,7,8 During the decade of 1970s the pediatric echocardiographic activity in Lund was intense with several meetings and many publications.
The work on cardiac ultrasound was based on a thirty-year-long collaboration between Inge Edler and Hellmuth Hertz, two quite different personalities. Dr. Inge Edler was technically curious, reflective, and a more practical clinician. Professor Hellmuth Hertz was younger, impulsive, with a drive for immediately trying new ideas and with an impressive heredity in the field of physics (Figure 3). Several times they were nominated for the Nobel Prize in Medicine and Physiology but no prize had yet been awarded for work on medical ultrasound. In 1977, the Albert Lasker Clinical Medical Research Award, “the American equivalent to the Nobel Prize in Medicine” was jointly shared between Inge Edler and Hellmuth Hertz both in Lund, Sweden. They received this for their pioneering work with “clinical application of ultrasound as a non-invasive tool in the medical diagnosis of abnormalities of the heart, probably the most important noninvasive tool for cardiac diagnosis since the electro-cardiography machine (Edler) and the development of technology in medicine (Hertz).”5
References
- Edler, I. Early echocardiography. Ultrasound in Med. And Biol., 1991; 17, 425-431
- Edler, I and Hertz, CH. The use of the ultrasound reflectoscope for continuous recording of the movements of heart walls. Kungl. Fysiogr Sällskap i Lund Förhandl 1954; 24(5): 40-58 (reproduced in Clin Physiol Funct Imaging (2004) 24: 118-136
- Edler, I. Ultrasoundcardiography. Acta Med Scand 1961;170 (suppl.370): 5-124
- Persson, S, Eskilsson, J and Lundström, N-R. The development of echocardiography in Sweden. Ultrasound in Clinical Diagnosis. Oxford University Press. 2012, 8-20
- Westling, H. Ultrasound in Lund- three world Ultrasound in Clinical Diagnosis. Oxford University Press. 2012, 1-7
- Lundström, N-R. Ultrasoundcardiographic studies of the mitral valve region in young infants with mitral atresia, mitral stenosis, hypoplasia of the left ventricle and cor triatriatum. Circulation, 1972; 45: 324-334
- Lundström, N-R. Echocardiography in the diagnosis of congenital mitral stenosis and in evaluation of the results of mitral valvotomy. Circulation, 1972; 46: 44-54
- Lundström, N-R. Echocardiography in the diagnosis of Ebstein’s anomaly of the tricuspid valve. Circulation, 1973; 47: 597-605
GÖRAN WETTRELL, MD, PhD, FLS, is an Associate Professor and Senior Consultant in Pediatric Cardiology and Pediatrics at Lund University, Sweden with interest in molecular genetics and primary arrhythmias. Other interests include male choir singing, travelling and medical history of pediatric cardiology and pediatrics.
Leave a Reply