
JMS Pearce
Hull, England

{kind=link}
“Fortiter in re, suaviter in modo (powerfully in deed, gently in manner).”
— Franz Nissl’s description of Alzheimer (1916)
Curiously, until the 1970s the high prevalence Alzheimer’s disease was not recognized as the most common cause of dementia.1 Most demented patients until then were labeled as having cerebral arteriosclerosis, or as sufferers from the inescapable wages of aging.
Alois Alzheimer
Alois Alzheimer (1864–1915) (Fig 1) was born the son of a Catholic notary in Marktbreit-am-Main. He attended medical schools in Berlin, Wurzburg, and Tubingen, graduating MD in 1888 and becoming an internist at Frankfurt.2 He was joined by Franz Nissl (1860-1919) with whom he enjoyed a lifetime collaboration. (Nissl developed the first (Nissl) stain of nerve cell structure.)
Alzheimer devoted his attention to the pathology of general paralysis for the insane (GPI), which was the subject of his post-doctoral thesis, “Histological Studies on the Differential Diagnosis of Progressive Paralysis” [GPI] to the University of Munich in 1904.
It was therefore no surprise when in 1894 Alzheimer received a telegram from his colleague Wilhelm Erb (1840-1920), asking for help with his patient Otto Geisenheimer, a banking director, who while in Algeria suffered a crisis of GPI. Alzheimer hurried to Algeria, but his efforts were in vain. However, Geisenheimer’s widow, Cecile, only weeks after her husband’s death, asked Alzheimer to marry her; they had three children. After Cecile’s death in 1901, Alzheimer moved to Heidelberg to join Emil Kraepelin and his colleague Nissl in 1902. He subsequently followed Kraepelin to the Anatomisches Laboratorium in Munich in 1904.3 Like his contemporaries, Emil Kraepelin (1856-1926), known as the Pope or the Linnaeus of Psychiatry, expressed skepticism about neuropathology to Oskar Vogt: “Anatomy can contribute nothing to psychiatry.”4 Alzheimer was to change his opinion.
He contributed both as clinician and pathologist not only to the organic basis for dementia, but to syphilis, arteriosclerosis, alcoholism, Huntington’s chorea, and epilepsy. A popular teacher and a meticulous, honest observer, he worked tirelessly, teaching and poring over the microscope, a cigar forgotten and unfinished on his bench. As he moved to the next student another cigar was lit and quickly placed at his side, by the end of the day twenty or more cigar stumps were strewn around the laboratory. Alzheimer’s sense of fun and humor on occasion caused him to dress up as a ballerina in a pink leotard and tutu for a carnival, or to disguise himself as a peddler carrying a tray of toys to amuse his young patients.
He eventually persuaded his mentor Kraepelin of the importance of clinicopathological correlations in psychiatry. He was appointed professor of psychiatry in Breslau in 1912, but on arrival was stricken with cardiac symptoms that delayed the start of his work. During World War I his longstanding rheumatic heart disease gradually worsened, and he died in 1915, aged fifty-two.
Alzheimer’s disease
Before Alzheimer, Pinel (1745-1826) and Esquirol (1772–1840) had separated dementia from other mental illnesses, but its organic basis and varied pathology were not defined. Blocq and Marinesco in 1892 had reported plaques in an epileptic patient without relating them to dementia. In 1907, the year of Alzheimer’s second report, Oskar Fisher described neuritic plaques in senile dementia.
While working in Frankfurt, Alzheimer studied the now famous fifty-one-year-old patient Frau Auguste Deter (1850–1906), known as Auguste D’. She had sought his help because her family had noticed that she had become uncharacteristically jealous of her husband, confused, forgetful, and frequently got lost. She was fortunate to end up in his hands in November 1901.
Auguste Deter (Fig 2)
A woman, 51 years old showed jealousy toward her husband as the first noticeable sign of the disease. Soon a rapidly increasing loss of memory could be noticed. She could not find her way around in her own apartment. She carried objects back and forth and hid them. At times she would think that someone wanted to kill her and would begin shrieking loudly. In the institution her behavior bore the stamp of utter perplexity. . . . Periodically she was totally delirious, dragged her bedding around, called her husband and her daughter, and seemed to have auditory hallucinations. . . . The generalized dementia progressed however. . . . After four and a half years of the disease death occurred. At the end, the patient was completely stuporose; she lay in her bed with her legs drawn up under her . . .
He was working in Munich when she eventually died in 1906, and her brain was sent to him. He reported her autopsy to a conference in Tübingen, on November 3rd and 4th, 1906.5 This landmark paper is still frequently quoted. He published a further report in 19076 and a more comprehensive review in 1911.7
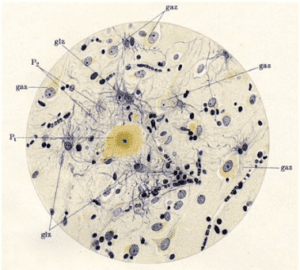
Auguste died of septicemia owing to infected decubitus ulcers. At autopsy Alzheimer found a generally atrophic brain without macroscopic lesions. Using Bielschowsky’s silver stain he described:
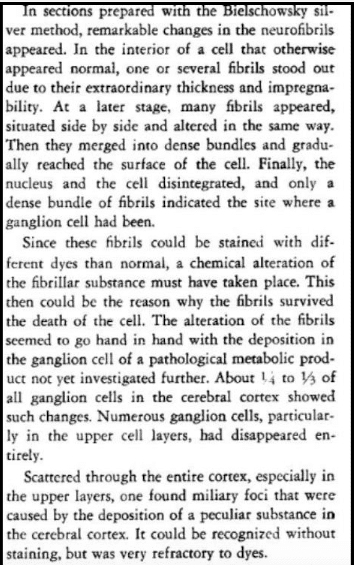
Later these changes were called respectively neurofibrillary tangles and amyloid plaques (Fig 3). Alzheimer did not claim that he had found a new disease.5 He was impressed by the variation of the neuropathological process, which he did not yet understand. What he did importantly demonstrate was that a degenerative process with resulting loss of essential neurons and atrophy of the brain could cause a decline in mental functions that constituted dementia. He was keen to show the value of newer histological techniques in delineating organic brain diseases that caused mental illnesses—a relatively new idea.
A year later, his colleague Francesco Bonfiglio (1883-1966) published another case, and two years later another. Gaetano Perusini (1879-1915) described four cases: two were the cases described by Alzheimer and Bonfiglio. They too believed that they had observed an unusual variant of senile dementia. Kraepelin introduced the term “Alzheimer’s disease” in the eighth edition of his textbook Compendium der Psychiatrie (1910). He knew of both Alzheimer’s and Perusini’s cases. He thought that these four patients were significantly different from the usual senile dementias; therefore he categorized them as presenile dementia. Alzheimer did not agree with this differentiation. Thus began a lasting dilemma: Was Alzheimer’s disease the same as, or was it a variant of senile dementia? Was the disease he had observed simply an aging process, or was there some other degenerative factor in operation?8 However, many people have normal cognitive function despite the presence of amyloid plaques.
The patient Johann F. whom he described in 1911 showed no neurofibrillary tangles, and Alzheimer was uncertain as to the role of plaques and neurofibrillary tangles in dementia. He had found they were sometimes inconspicuous in patients with severe dementia, and he probably observed them in some normal brains.
The archive of Auguste D’ was lost for many years. It was discovered in the archives of the Goethe University Hospital in Frankfurt and the original brain samples from Auguste D’ and Johann F were re-examined. Auguste D’s brain contained no vascular changes, but numerous plaques and tangles, the classic signs of Alzheimer’s disease. Her APOE genotype was shown to be E3/E3.9 Johann F had plaques but no tangles; he was homozygous for the apolipoprotein allele epsilon3 and lacked specific APP mutations.10
————
Alzheimer‘s disease now covers both the presenile and senile forms.11 Plaques are composed of degenerating nerve cells surrounding deposits of the protein amyloid beta (Aβ amyloid). This is derived from amyloid precursor protein (APP) that plays a role in neuronal growth and neurotoxicity.12 Neurofibrillary tangles are twisted fibers of a protein called tau that normally occurs in neurons, but in diseased states tau molecules clump together and form tangles, and also the inclusion bodies in Pick’s and Lewy body diseases.
Alzheimer disease is a genetically heterogeneous disorder associated with the APOE4 allele on chromosome 19 caused by mutation in the presenilin-1 gene (PSEN1) on 14q; and caused by mutation in the PSEN2 gene on 1q31. There is evidence for additional AD loci on other chromosomes. Mutations in presenilin-1 and -2 are the major associations with the rare, early-onset familial Alzheimer’s disease (FAD). The presence of the apolipoprotein E4 allele on chromosome 19 is a risk factor for late-onset AD.13 There is also evidence of an AD susceptibility locus on chromosome 12 and possibly on other chromosomes.
Since several drugs that reduce the levels of Aβ amyloid peptide within plaques have consistently failed to improve the clinical features or relentless progression, the relationship between plaques and dementia remains in doubt. Similarly, only slight and ill-sustained benefit attends the surprisingly common prescriptions for the acetylcholinesterase inhibitors donepezil and rivastigmine, or the glutamate blocker memantine.
Other common causes of dementia
Alzheimer’s work led to the wider recognition of many other causes of dementia, for example tumors or severe brain trauma. Arnold Pick (1851-1924) in 1902 had described a senile dementing illness characterized by frontal lobar atrophy and “Pick bodies,” which is now grouped with the “fronto-temporal dementias.” Friederich Lewy (1885-1950) in 1912 working in Alzheimer’s laboratory discovered cytoplasmic inclusions in Parkinson’s disease brains; subsequently diffuse Lewy bodies were found in certain patients with characteristic early hallucinations, fluctuating dementia, and Parkinsonism, known as diffuse Lewy body disease. Alzheimer recognized vascular dementia and gave the first account of the lacunar infarcts in Binswanger’s “subcortical arteriosclerotic encephalopathy.” Vascular dementia is regarded as a common cause of dementia, separate from but often coexisting with Alzheimer’s disease; its definition remains imprecise. Because some benign tumors, metabolic disorders, and certain infections of the brain are potentially reversible, dementia at any age requires investigation.
Additional biography
- Hoff P. Alois Alzheimer 1864-1915. [An overview of his life and work on the occasion of his 125th birthday]. Nervenarzt. 1989;60:332-7.
- Kircher T, Wormstall H. Alois Alzheimer (1864-1915)–student days and first scientific activities. J Geriatr Psychiatry Neurol 1997;10:127-9
- Maurer K and Maurer U. Alzheimer: the life of a physician and the career of a disease (1998), translated Neil Levi and Alistair Burns. Columbia University Press, 2003.
- Pérez-Trullén JM. A Brief Biography of Alois Alzheimer. Neurosciences and History 2013; 1(3): 125-136.
References
- Pearce JMS. Clinical Aspects Of Dementia. London, Bailliere Tindall 1973.
- Hoff P. In: Berrios GE, Freeman HL (eds). Alzheimer and the Dementias. London, Royal Society of Medicine Services Ltd. 1991.
- Goedert M, Ghetti B. Alois Alzheimer: his life and times. Brain Pathol. 2007;17(1):57-62.
- Lewey FH. Alois Alzheimer. In: Haymaker W and Schiller F, eds. The Founders of Neurology. eds. 2nd edn. Springfield. Charles C Thomas pp. 315-8. 1970.
- Alzheimer A. Uber eine eigenartige schweren.Erkrankung prozeb der Hirnrinde. Neurologisches Centralblatt 1906;23:1129–1136. Transl in Arch Neurol 1969;21:109-110.
- Alzheimer A Uber eine eigenartige Erkrankung der Hirnrinde. Allgemeine Zeitschrift fur Psychiatrie und Psychisch- Gerichtliche Medizin 1907;64:146–148.
- Alzheimer A. Über eigenartige Krankheitsfalle des späteren Alters. Z die Gesamte Neurologie Psychiatrie 1911;4: 456– 385.
- Arts NJM. Alzheimer’s Disease In: Koehler PJ, Bruyn GW, Pearce JMS. Eds. Neurological Eponyms. Oxford, OUP 2000.
- Graeber MB, Kösel S, Grasbon-Frodl E, Möller HJ, Mehraein P. Histopathology and APOE genotype of the first Alzheimer disease patient, Auguste D. Neurogenetics. 1998 Mar;1(3):223-8.
- Graeber MB, Kösel S, Egensperger R, Banati RB, Müller U, Bise K, Hoff P, Möller HJ, Fujisawa K, Mehraein P. Rediscovery of the case described by Alois Alzheimer in 1911: historical, histological and molecular genetic analysis. Neurogenetics. 1997 May;1(1):73-80.
- Pearce JMS. Alzheimer’s disease. Journal of Neurology, Neurosurgery & Psychiatry 2000;68:348.
- Sheng JG, Zhou XQ, Mrak RE, Griffin WS. Progressive neuronal injury associated with amyloid plaque formation in Alzheimer disease. J Neuropathol Exp Neurol. 1998; 57: 714-7.
- Wisniewski T, Dowjat WK, Permanne B, Palha J, Kumar A, Gallo G, Frangione B. Presenilin-1 is associated with Alzheimer’s disease amyloid. Am J Pathol. 1997; 151: 601-10.
JMS PEARCE, MD, FRCP, is emeritus consultant neurologist in the Department of Neurology at the Hull Royal Infirmary, England.