
Jennifer Evans
Sara Read
United Kingdom
The early modern body was thought to be composed of and ordered by an intricate balance of fluids, the most important of which was blood. Blood was universally understood to have two origins: the heart and the liver. Together with the brain, these organs formed what Galen called “the noble organs.” Ideas about the origins of blood changed when in the 1620s William Harvey, physician at the Stuart court, conducted a series of experiments on live animals to prove that in fact the body had one circulation system. Blood was produced in the liver and pumped around the body in a continuous circuit. However, although his findings were published as Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus in 1628, the new theory took a while to be integrated into medical practices and the true implications of Harvey’s work only became known years later.
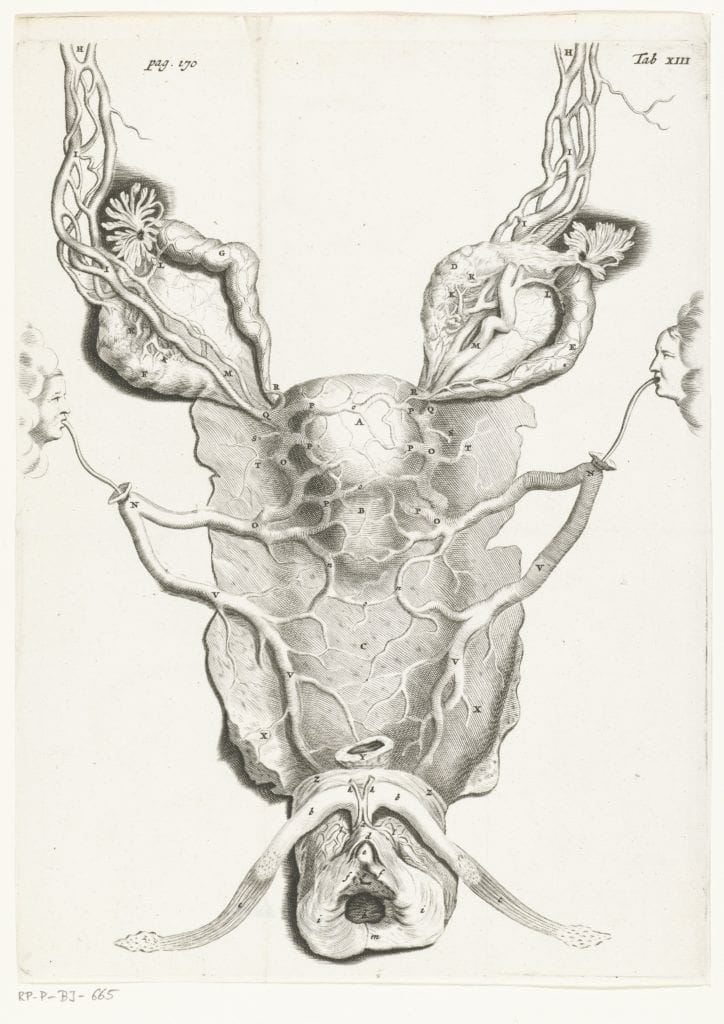
Blood did not only pulse around the body in its fundamental form but was transformed through the process known as “concoction” into fat, sweat, seed, and milk.1 Thus, Richard Griffith in 1681 was able to ask rhetorically, “[w]hat thing is there in nature approaches nearer to an Identity with Blood, than Milk doth?” adding a codicil that one should disregard the change in “Colour and some few accidental Differences.”2 This process happened in the mother’s breast after parturition. As the popular medical text Aristotle’s Master-piece told readers, “the milk is nothing but the menstruous blood made white in the brests.”3 Men’s supposed hot temperaments meant that their excess blood was transformed into sweat and released from the body or concocted into semen and expelled to create new life. Women’s excess of blood was converted into a fatty layer beneath the skin and was expelled from the body each month through menstruation. If a woman became pregnant this blood was used to nourish the developing fetus in her womb, and so menstruation ceased. After birth, menstrual blood was diverted through a conduit, variously described as a duct or vein, to the breasts where it was concocted into breastmilk to allow for the continuing support and development of the infant.4 This is demonstrated in an early anatomical drawing by Leonardo da Vinci from the 1490s, which shows a vein directly running between the womb and the breast.5 The anonymously authored seventeenth-century Physical Dictionary stated that “Mamillary veins: [were a] passage from the Womb to the breasts, serving to convey the menstrual bloud thither.”6 This connection was described well into the eighteenth century, when John Maubray detailed how the breasts contained two sorts of veins: the common veins branched from the vena cava and supply the nutrition for the breasts themselves, whereas the mammary veins carried blood directly from the womb, via a connection with the “epigastrick” veins.7
One of the effects of Harvey’s work on the next generation of physicians was to problematize the accepted wisdom that milk was blood made white. As Thomas Gibson wrote in his 1682 anatomy guide: “It was an old opinion that Milk was made of Bloud sent from the Womb by the Epigastrick vessels ascending, and as was thought inosculating with those branches of the Mammariae that descend towards the Navel.”8 But Harvey’s work and later dissections showed that this anatomical assumption was flawed “so it is generally denied that either Bloud sent from the Womb, or from wheresoever, is the true matter out of which Milk is made.” For Gibson, the key point was that the blood-to-milk theory meant “the Mother could every day endure the loss of so much Bloud (suppose a pound and half) as the Child sucks daily Milk from the Breasts” which, as he argues, would be quite incredible. However, despite claims this was an outmoded opinion, medical writers like John Maubray continued describing it well into the eighteenth century.
Beyond theoretical discussions, the idea of a connection between women’s blood and milk retained potency in medical practice as one case-note from Staffordshire physician Richard Wilkes shows. He recorded attending “one Mrs Parkes of Wtampton [sic] who had been deliver’d of 2 Children on ye 16th 1739 she had violent Pains in her Belly; wch kept her waking all Night the Lochia were intirely stopt.”9 He determined the lack of postpartum bleeding resulted from the fact “her Milk came in 24 Hours after Delivery & flow’d in great Quantity.” “[S]trong Emmenagogic Medicines” failed to encourage the lochial bleeding to return, but since the woman was well when he checked four days later, he saw no cause for further intervention.
Since this conversion of blood to milk occurred after parturition, milk or blood appearing in the breasts at the wrong time could indicate an impending miscarriage. As German physician Michael Ettmüller explained, “Hippocrates look’d upon the flagginess and Extenuation of the Breasts, or their voiding of Milk or Blood, as a sign of miscarrying.”10 Likewise, Aristotle’s Master-piece told readers that a sign “of future Abortion” was “a Flux of waterish Milk,” which again suggested a failure to successfully transmute blood to milk.11 Leaking of milk from the breasts indicated that the body was no longer using blood in the uterus to nourish a fetus and so had sent it to the breast before they were ready to effect this transformation.
In some cases, the mother’s body failed to transform blood once the baby had been born. On 25 January 1739 Wilkes attended a new mother and her young son who had “puked up” blood.12 After assessing the infant, Wilkes realized that the blood was not from the child’s body but was regurgitated feeds. He had been consuming blood, not breastmilk from his mother’s breasts. The mother’s supposed failure to “concoct” her menstrual blood into suitable nourishment for the baby meant he had to be weaned.
Wilkes did not mention any attempts to bolster the woman’s ability to transform blood into milk. Yet medical remedies designed to increase a woman’s production of breast milk often noted the link between blood and the absent milk. One mid-seventeenth century text, The Skilful Physician, explained:
If a woman want milk in her Brests. The cause may be of heat or drowth, or of some cold quality of the brest, that the blood which should alter into milk be dryed out. Again, the want of milk, may be for want of meat, or use of such meats as may dry the blood; or by bad digestion of the stomack, &c. use a good Diet, and eat green Marjerom in the morning fasting.13
One reason a woman might lack milk was because she had become sexually active too soon after the birth. Théophile Bonet instructed readers, “Let the Nurse wholly abstain from Venus, for it disturbs the Milk, draws the Bloud to the Womb, whereby the Milk is spoiled, and the quantity of it abated.”14 If the fungible blood was attracted back to the womb because of the heat and agitation of intercourse, then it was not available to be transformed into milk in the breast. Bonet was clearly alert to the fact that a woman denying her husband sex could cause strained marital relations and so described an exception to this rule, “Yet Varandaeus [Jean Varandal of Montpellier] allows it to such as live with their Husbands, lest their longing disturb them. And we see Mothers, who live with their Husbands, and lye with them, do yet suckle their Children without any harm.”15 Implicit in this instruction, therefore, is that the advice was essential for wet-nurses but not for mothers nursing their own babies.
Conversely, as the midwife Jane Sharp explained to readers of her 1671 treatise, women suffered during breastfeeding if there was too much milk and the child was “not able to suck it all.” This, she detailed, led to imposthumes (abscesses) and the breasts would swell, grow red, and become painfully overstretched.16 Sharp was clear that “too much blood is the cause of it.” The remedy was that the “woman must eat and drink with moderation, and use a drying diet,” which would limit the creation of blood in the body and so limit the amount of milk transformed from the same.
As has been demonstrated within the humoral system where fungible fluids transformed and flowed around the body, breastmilk had to be regulated and kept in balance as if it were indeed blood made white.
References
- ‘Concoction’: Ripening, maturing, and bringing to a state of perfection www.oed.com (14.10.19).
- Richard Griffith, A-la-mode Phlebotomy No Good Fashion (London, 1681), 40.
- Anon., Aristotle’s Master-piece (London, 1702), 98.
- Victoria Sparey, “Identity-Formation and the Breastfeeding Mother in Renaissance Generative Discourses and Shakespeare’s Coriolanus,” Social History of Medicine, 25, no. 4 (October 2012), 777.
- This drawing is reproduced in Mathew Cobb, The Egg and Sperm Race (London: Free Press, 2006), 8.
- Anon, A Physical Dictionary, or, An Interpretation of such crabbed words and terms of arts, as are deriv’d from the Greek or Latin (London, 1657), I3.
- The Female Physician, Containing All the Diseases Incident to that Sex in Virgins, Wives and Widows (London, 1724), 41. Normally these are just referred to as menstrual veins.
- Thomas Gibson, The Anatomy of Humane Bodies Epitomized (London, 1682), 216.
- Richard Wilkes Observations Volume 2, MS 5006, Wellcome Library, London, 5.
- Etmullerus Abridg’d: or, A Compleat System of the Theory and Practice of Physic (London, 1699), 616.
- Anon., Aristotle’s Master-piece (London, 1702), 155.
- Wilkes, Obsevations, 5.
- Bahia Secretaria das Minas e Energia, The Skilful Physician (London, 1656), 59-60.
- Théophile Bonet, A Guide to the Practical Physician (1686), 322.
- Bonet, Practical Physician, 322.
- Jane Sharp, The Midwives Book (London, 1671), 338.
JENNIFER EVANS, PHD, FRHistS, is a Senior Lecturer in History at the University of Hertfordshire, UK and SARA READ, PHD, FRHistS, is a Lecturer in English, Loughborough University, UK. Dr. Evans and Dr. Read focus their individual and joint research around the cultural history of the reproductive body in early modern England. Their previous research has resulted in monographs on the use of aphrodisiacs as fertility aids (Evans, 2014) and menstruation and related female bleeding (Read, 2013). They jointly authored an academic article “’Before Midnight she had Miscarried’: Men, Women and Miscarriage in Early Modern England” (Journal for Family History 40.1 (2015)). Most recently, they published a popular history book Maladies and Medicine: Exploring Health and Healing, 1540-1740 (2017) and run the blog earlymodernmedicine.com.
Submitted for the 2019–2020 Blood Writing Contest & Highlighted in Frontispiece Volume 12, Issue 2 – Spring 2020