
Alan Jay Schwartz
Philadelphia, Pennsylvania, United States
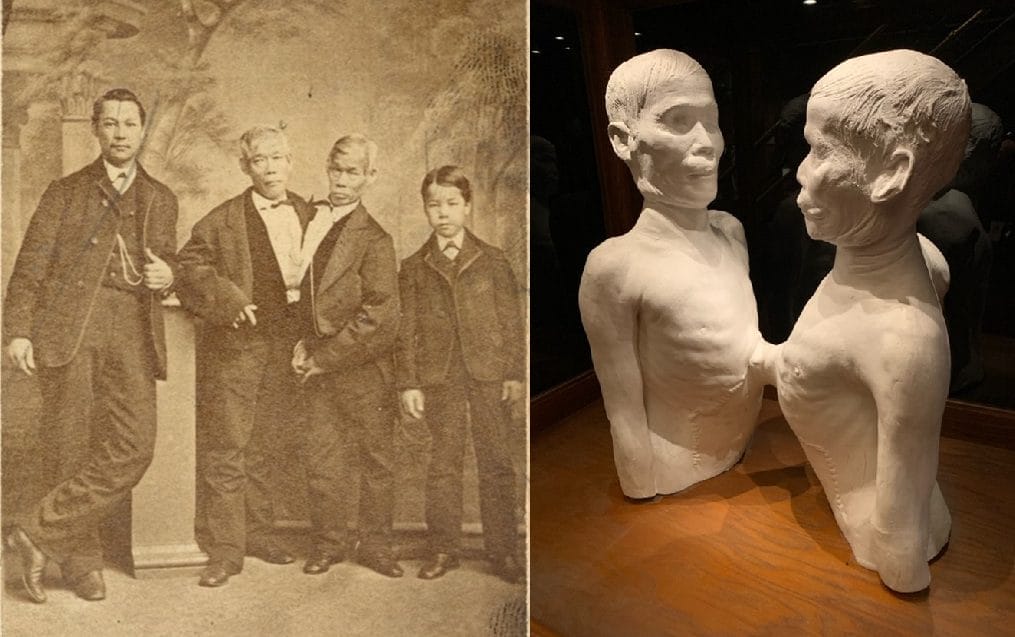
b. Plaster cast of the joined torsos of Chang and Eng. Photo by Lowell Flanders, courtesy of the College of Physicians of Philadelphia.
Conjoined twins present a rare and challenging occurrence. With an incidence of 1 per 50,000–200,000 births,1 the successful separation of conjoined twins is a phenomenal medical-surgical challenge.2 Two reasons, among others, explain why such separation has become successful: a) detailed visualization of the pathologic anatomy and b) simulating and practicing clinical separation scenarios. Consider two sets of conjoined twins, living more than 150 years apart, that exemplify this medical-surgical advance.
In their lifetime, Chang and Eng Bunker (1811–1874) were individuals with uncharted pathologic anatomy. These brothers were xiphopagus conjoined twins (Fig 1a). Their livers were connected at the sternum. Chang and Eng were born in Siam (thus giving rise to the term “Siamese twins”) and brought to the United States in 1829. Their curiosity was financially exploited for a decade through displaying them, for the cost of a ticket, at “freak shows.” Tired of this demeaning and onerous existence, they ended touring, married, and ultimately fathered 21 children. For a brief time in 1860, they signed with P.T. Barnum and were exhibited in Barnum’s American Museum. In 1870, Chang suffered a stroke. He died three years later, and Eng succumbed eight hours after Chang.
Until they died, physicians could only speculate about anatomic structures that linked the brothers. Autopsy retrospectively delineated the anatomic fact of the fused ligament connecting their sterna. Prior to their interment, doctors memorialized what, until the deaths of the twins, they only surmised. The unusual anatomy was photographed. The Bunkers’ fused livers were preserved. Their joined torsos were commemorated by a plaster cast (Fig 1b). The livers and plaster cast continue to be displayed at the College of Physicians of Philadelphia.
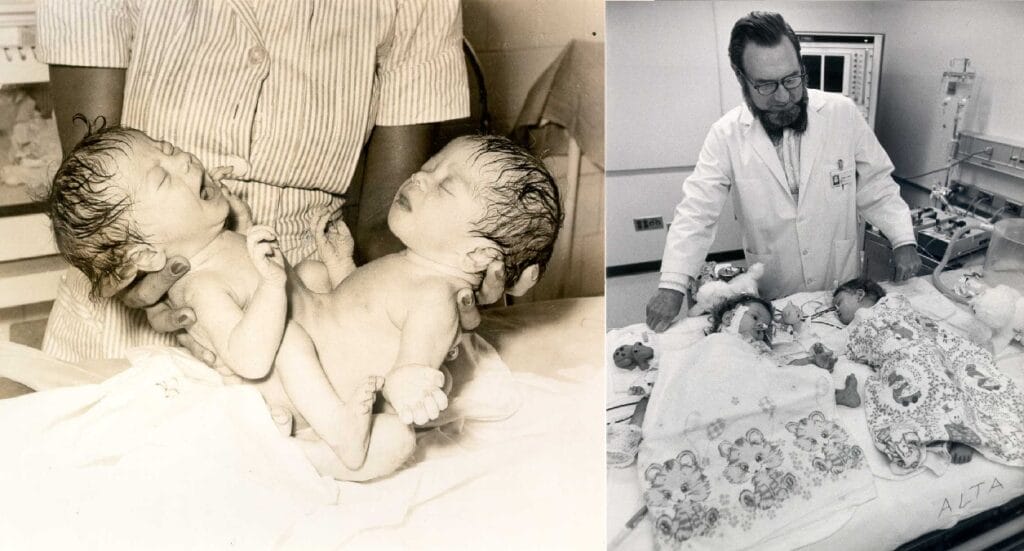
b. Dr. C. Everett Koop with the successfully separated Rodriguez twins. 1974.
Photos via the National Library of Medicine.
Fast forward to 1973, 100 years after the death of Chang and Eng. Clara and Altagracia (Alta) Rodriguez, ischiopagus twins, joined together at the lower trunk and pelvis (Fig 2a) were born in 1973, in the Dominican Republic. In September 1974, C. Everett Koop, MD (1916–2013; Surgeon-in-Chief at the Children’s Hospital of Philadelphia [CHOP] 1948–1981) directed a team of 26 doctors and nurses during an 8-hour surgery to successfully separate the Rodriquez twins (Fig 2b).4
What distinguishes the successful 1974 separation from the lack of an attempt to separate Chang and Eng in the mid-1800s? Advances in medical imaging techniques and presurgical clinical simulation exercises, among other factors, explain the 100-year difference.
As the surgical team from CHOP reviewed their modern-day experience caring for 13 conjoined twins,4 they credited accurate imaging as a key determinate of successful separation and survival of the patients. Advances in imaging have enabled everyone involved in a possible separation to envisage the anatomic facts. Chang and Eng were cared for by physicians who could only speculate about how the twins were connected, and not knowing the anatomy made it impossible to devise a surgical plan. Modern imaging techniques5-8 changed that deficiency. Procedures including and not limited to X-ray, computed tomography, ultrasound, radionuclide marking, angiography, and 3D printed models gave healthcare practitioners “eyeglasses” to develop surgical “roadmaps” while protecting critical organs and structures.
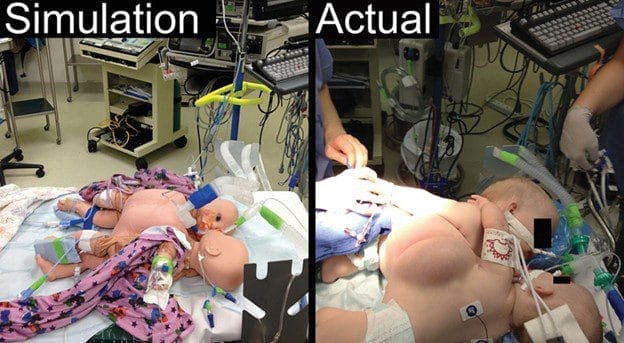
Effective and safe surgical separation of conjoined twins, enabled when seeing their anatomy became a reality, was augmented by presurgical clinical simulation. Such a surgery is analogous to flying a jumbo jet; pre-flight preparation, flight operation risks, in-flight awareness, and contingencies for unexpected events and emergencies make split-second decisions necessary. Borrowing the flight simulation training model, surgery simulation has gained popularity as an effective and riskless technique to prepare providers.9,10
While conjoined twin separation surgery is both extremely complex and exceedingly rare, simulation offers a variety of logistics in how to prepare surgically and to accomplish the myriad steps that nursing, surgical, and anesthesia personnel must perform. Teamwork principles (e.g., leadership and communication) can be practiced and enhanced by the use of simulation to ensure the optimization of team synergy and to ensure safe, effective patient care.10 (Fig 3)
While many medical-surgical problems exist relatively unchanged over time, care for this particular malady has evolved and improved. Exploring the historical evolution and time-dependent context of medical-surgical care enlightens one’s grasp of what were once obstacles, turning them into therapeutic triumphs.
References
- Edmonds LD, Layde PM. Conjoined twins in the United States, 1970-1977. Teratology 1982;25:301-8.
- Fischer H. Dr. Doyen separates conjoined twins in 1902. Hektoen International Birth, Pregnancy, & Obstetrics, Summer 2022. https://hekint.org/2022/07/25/dr-doyen-separates-conjoined-twins-in-1902/. Accessed April 18, 2025.
- O’Neill J, Holcomb GW, Schnaufer L, Templeton J, Bishop H, Ross A, Duckett JW, Norwood WI, Ziegler MM, Koop CE. Surgical Experience with Thirteen Conjoined Twins. Ann Surg, 1988:208(3);299-312.
- From ‘Monsters’ to Modern Medical Miracles: Selected moments in the history of conjoined twins from medieval to modern times. US National Library of Medicine March 11, 2024. https://www.nlm.nih.gov/hmd/conjoined/separation.html. Accessed April 25, 2025.
- Miller D, Colombani P, Buck JR, Dudgeon DL, Haller JA. New Techniques in the Diagnosis and Operative Management of Siamese Twins. J Pediatr Surg 1983:18;373-6.
- Mann MD, Coutts JP, Kaschula ROC, Fraser CB, Fisher RM, Cywes S. The Use of Radionuclides in the Investigation of Conjoined Twins. J Nucl Med 1984:24;479-84.
- Marcinski A, Lopatec HU, Wermenski K, Wocjan J, Gajewski Z, Kaminski W, Dura W. Angiographic Evaluation of Conjoined Twins. Pediatr Radiol 1978:6;230-2.
- Rodriguez-De-Velasco A, Apaza JL, Rojas N, Martinez P, Padilla-Huamantinco P, Zuñiga JM, Jaramillo-Cañas W, Tincopa JP, Quispe-Juli CU. Surgical planning and separation of ischiopagus conjoined twins using 3D printed models and intraoperative neurophysiological monitoring. J Pediatr Surg Case Reports 2023:92;102604.
- Murray AW, Beaman ST, Kampik CW, Quinlan JJ. Simulation in the Operating Room. Best Practice & Research Clinical Anaesthesiology 2015:29;41-50.
- Simpao AF, Wong R, Ferrara TJ, Hedrick HL, Schwartz AJ, Snyder TL, Tharakan SJ, Bailey PD. From Simulation to Separation Surgery—A Tale of Two Twins. Anesthesiology 2014;120;110.
ALAN JAY SCHWARTZ, MD, MSEd, received his BA and MD from Temple University and his MSEd from the University of Pennsylvania. He is retired having practiced cardiac and pediatric anesthesiology at the University of Pennsylvania and Children’s Hospital of Philadelphia (CHOP) where he was the Pediatric Anesthesia Fellowship Director. He is a Docent at the Mütter Museum of The College of Physicians of Philadelphia.