
Richard de Grijs
Sydney, Australia
The often awe-inspiring works of art immortalizing historic naval battles usually belie the harsh reality of war. Amidst clouds of billowing, black smoke and the deafening roar of cannon fire, sailors faced the real danger of life-threatening injuries.
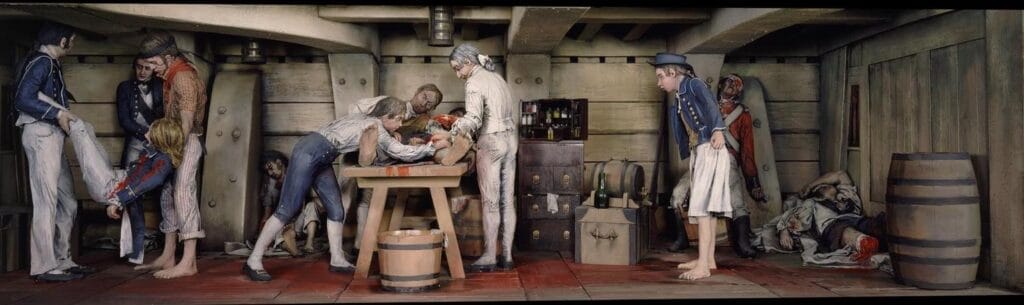
Injured sailors were carried, dragged, or stretchered to the surgeon’s “cockpit,” a dimly lit, low-ceilinged, and overcrowded space usually home to the midshipmen, and located toward the stern on the orlop (lowest) deck. They were then placed on makeshift operating tables composed of the midshipmen’s assembled sea chests, which were often simply covered with an old sail or other cloth. Conditions were nightmarish, with treatment frequently interrupted by desperate cries for relief:
The first object I met was a man bearing a limb, which had just been detached from some suffering wretch … The surgeon and his mate were smeared with blood from head to foote: they looked more like butchers than doctors …1
Although most shipboard infirmaries were located in relative safety below the waterline, the surgeon’s job was not without danger:
[The patient] was laid on the table and the operation performed in the usual way …, lucky it was that he bare [sic] it so well, as a shot at this time came into the cockpit and passed the operating table close, this startled all the women who formed the chief of my assistance.2
Although this particular incident at the Battle of Camperdown (October 11, 1797) did not cause any additional distress, patients were not always spared from further injury, or even death:
As I was dressing a wounded man, a cannon ball struck a young gentleman on the head dashing his brains upon all sides; part of them blinded me. At this moment a splinter struck my head and rendered me insensible for [a] quarter of an hour. Upon my recovery, I could hardly persuade myself but what I was mortally wounded, from being completely besmeared with blood and brains.3
Whereas national navies routinely mustered qualified doctors, medical care on merchant vessels often relied on surgeons rather than physicians. Physicians were usually well-educated but lacked practical experience; (barber-)surgeons were proficient in treating common shipboard injuries.4 During naval battles, “amputation was the most common operation, along with sewing up abdominal wounds.”5 If no surgeon was available, amputations were usually performed by the ship’s carpenter—or even by the cook.
Surgeons were assisted by a surgeon’s mate, a “loblolly boy,” and occasionally by additional assistants.6 Loblolly boys collected amputated limbs, poured sand onto blood-soaked, slippery surfaces, and prepared buckets of cauterizing tar. Their nickname referred to the thick meat and vegetable porridge (“spoon meat”) they fed the sailors in their care;7 their modern counterparts are the U.S. Navy’s hospital corpsmen or the Royal Navy’s medical assistants.
When required, they would also immobilize patients by any means necessary so that the surgeon could do his job. In Of Wounds, Severall Chirurgicall Treatises (1676), Richard Wiseman (1622?–1676) explains:
At Sea they sit or lie, I never took much notice which; nor do I remember I had ever any body to hold them; but with the help of my [Surgeon’s] Mates, and some one or two that belonged to the Hold, I went on with my work.8
Despite Wiseman’s dispassionate reference to the need for his assistants to restrain his patients during amputations, having access to such support was by no means a luxury. General anesthesia was not routinely administered until the mid-nineteenth century,9 and amputees were often in considerable pain:
We held [the patient] while the surgeon cut off his leg above the knee. The task was most painful to behold, the surgeon using his knife and saw on human flesh and bones as freely as the butcher at the shambles.10
A popular myth contends that patients requiring amputation were given copious amounts of “cordial” (rum) to numb the pain; however, they often only received a mouth guard, a simple stick to bite down on when their pain became unbearable. There is some evidence that “a drachm of Cordial [was] given to the man to keep up his Spirits.”11 And although “[t]he Operator is to encourage the Patient, and having given him half a Glass of Wine, to enable him the better to endure his Pain,”12 a patient’s spirit intake was usually limited to a single shot:
When you resolve to set upon this Operation [amputation], having all things necessary in a readiness upon a Table near you; first give the Patient a good Cordial, and encourage him by proper words, to suffer with patience what will conduce to his future well-being.13
In fact, to ease a patient’s pain post-operation, liberal consumption of alcohol was not recommended:
[The operation] done, let him have another Cordial drachm, but have a care of too much, lest it inflame him, and make his blood more fluid: And have an Eye lest his Messmates come with their bottle, and prejudice him with their kindness, as I have sometimes seen.14
Without anesthetic, amputees were often given opiates such as laudanum—opium blended into rum—which made them groggy and dulled the pain somewhat. But perhaps the most effective means of pain management was the natural adrenaline rush caused by the battle raging upstairs.15 This suggested that amputations should be performed “whilst the Blood is hot, and there is Strength; then [sic: rather than] afterward when the Fever or other ill symptoms are come on.”16 British Navy surgeon John Atkins (1685–1757) agreed:
Heat and Surprize in Action makes it the properest Time for amputating, Men meeting their Misfortunes with greater Strength and Resolution than when they had spent a Night under Thought and Reflection.17
Despite their training, many Royal Navy surgeons’ skills were not much more advanced than those of the common butcher. Their tools were also similar. As a case in point, the personal surgery kit of Alexander Jack, Royal Navy surgeon on HMS Shannon during the War of 1812, contained an amputating and a metacarpal saw (used to cut small bones), three amputating knives, two pairs of sliding artery forceps (for tying ligatures), three curved suture needles, two Petit’s screw tourniquets,18 bone forceps, and a hooked needle.19,20
Seventeenth- and eighteenth-century surgeons’ instrument sets usually contained several types of bladed tools, including serrated knives to saw through muscle; amputation or “capital” knives with smooth blades to slice away skin; curved tools, each for their own specific purpose; and usually also a thin, serrated bone saw.21 In the heat of battle and lacking anesthesia, surgeons had only limited time to complete an amputation and stop a patient’s hemorrhaging, so access to the right tools was paramount. Competent surgeons would perform amputations in less than two minutes, sometimes considerably more quickly. Speed was of the essence to avoid infection and sepsis; the quicker amputations were completed, the greater the patient’s chances of survival. Therefore,
… let the discreet Surgeon be ever prepared …, and to that end let the Dismembring saw be alwaies in readinesse, well filed, and cleane kept in oyly clouts [cloths] to save it from rust, let it also have two blades wel filed ere you put it into your chest, for that one tooth in a saw may breake.22
Although early naval surgeons cauterized their patients’ stumps with hot tar or a preheated iron to slow profuse bleeding, application of arterial vessel ligatures resulted in a much greater reduction in blood loss.23 Moreover, the use of hot pitch often turned lethal, hence that practice was soon abandoned. Renowned sea surgeon John Moyle (d. 1714) recommended to prepare a “large Tape [strip of material] for Ligature, and narrower for other occasions, [and] Cautrizing Buttons ready in the fire.”24 In turn, John Atkins explained:
We begin by fixing the tourniquet. And for this purpose, having drawn the muscles taut upwards, we enfold the thigh or arm with a thick linen compress … Besides these we fasten two other tape ligatures at the very place we are to make the amputation, leaving only room between them for the knife to got round. The use of these is to swell the flesh to the knife, and to guide it for a smooth circumcision which you are now to make, bringing it at once as near the bone as you can, and as far round. … The saw is to be set on both bones at once (if two) and divided at as few strokes as possible, taking heed in the division that the nearer you come through, the easier to move, lest the bones should splinter.25
In 1786, Lancelot Haire, assistant surgeon at Haslar Naval Hospital near Portsmouth (England), introduced an important improvement. He recommended that ligatures be cut short,26 a practice that helped to reduce infection. Moreover, the application of tourniquets—composed of a cloth strap and a screw—further reduced hemorrhaging. As a case in point, at the Battle of Santa Cruz de Tenerife (1797), Admiral Horatio Nelson (1758–1805) lost his right arm but owed his life to his nephew, Josiah Nisbet (c. 1780–1830), who quickly threw a tourniquet around the admiral’s severed limb to allow adequate compression and stop the hemorrhaging.27
The risk of complications and death from gangrene was high. Most surgical authors agreed that applying bandages28—often two “rounds” of linen drenched in vinegar and water—would act as effective antiseptic; egg whites were used to stem the bleeding. Although the mortality rate during naval battles was only around 5%, trauma-induced complications resulted in survival chances of just 10 to 50 percent.29 Hence, and contrary to popular opinion, amputations were the surgeon’s last resort, not his first choice.
Notes and references
- Estes, JW. Naval Surgeon: Life and Death at Sea in the Age of Sail. (Canton, MA: Science History Publications, 1998), 65.
- MacGrath, G. The Medical Journal of HMS Russel, between 30th May 1797 and 30th May 1798. PRO.ADM 101–118/1. London: Public Record Office.
- Lowry, J. Fiddlers and Whores: The Candid Memoirs of a Surgeon in Nelson’s Fleet. (London: Chatham, 2006), 44.
- State Library of New South Wales, 2022–2023. “Kill or Cure? A Taste of Medicine.” https://sl.nsw.gov.au/killorcure [accessed December 28, 2023].
- Druett, J. Rough Medicine: Surgeons at Sea in the Age of Sail. (New York: Routledge, 2001), 50–65.
- Kehoe, M. “The Pirate Surgeon’s Journals. Amputation During the Golden Age of Piracy.” https://www.piratesurgeon.com/pages/surgeon_pages/amputation3.htm [accessed December 28, 2023].
- U.S. Naval Institute. “A Brief List of Old, Obscure and Obsolete U.S. Navy Jobs,” updated Sept 5, 2016. https://news.usni.org/2014/12/03/brief-list-old-obscure-obsolete-u-s-navy-jobs [accessed December 28, 2023].
- Wiseman, R. Of Wounds, Severall Chirurgicall Treatises. (London: E. Flesher and J. Macock, 1676), 452.
- Morton, WTG. Remarks on the Proper Mode of Administering Sulphuric Ether by Inhalation. (Boston, MA: Button and Wentworth, 1847).
- Estes, op. cit.
- Moyle, J. Chirurgus Marinus: or, the Sea-Chirurgion. Being Instructions to Junior Chirurgic Practitioners, Who Design to Serve at Sea in This Imploy. (London: E. Tracy and S. Burrowes, 1702), 24.
- Dionis, P. A Course of Chirurgical Operations, Demonstrated in the Royal Garden at Paris, 2nd ed. (London: J. Tonson, 1733), 411.
- Kehoe, op. cit. https://www.piratesurgeon.com/pages/surgeon_pages/amputation4.htm [accessed December 29, 2023].
- Moyle, Chirurgus Marinus, 28.
- Kirkup, J. The Evolution of Surgical Instruments. An Illustrated History from Ancient Time to the Twentieth Century. (Navato, CA: historyofscience.com, 2006), 378.
- Moyle, J. Chyrurgic Memoirs: Being an Account of Many Extraordinary Cures Which Occurred in the Series of the Author’s Practice. (London: D. Browne, 1708), 118. See also Wiseman, op. cit., 420.
- Atkins, J. The Navy-surgeon: Or, a Practical System of Surgery. (London: Caesar Ward and Richard Chandler, 1734), 131.
- Hawk, AJ.. “ArtiFacts: Jean Louis Petit’s Screw Tourniquet.” Clinical Orthopaedics and Related Research, 474, (2016): 2577–2579.
- Almond, R. “The Anatomy Lab: Jack and the Shannon.” Surgeons’ Hall Museums, Edinburgh, 2016. https://surgeonshallmuseums.wordpress.com/2016/12/28/jack-and-the-shannon/ [accessed December 29, 2023].
- See also Woodall, J. The Surgions Mate, Or, a Treatise Discouering Faithfully and Plainely the Due Contents of the Surgions Chest. (London: Edward Griffin, 1617), 172; Atkins, op. cit., 123–124; Bruijn, I. Ship’s Surgeons of the Dutch East India Company: Commerce and the Progress of Medicine in the Eighteenth Century. (Leiden: Leiden University Press, 2009), 70–71.
- Sachs, M, Boujunga, J, and Encke, A. “Surgical History: Historical Evolution of Limb Amputation.” World Journal of Surgery, 23, (1999): 1088–1093; Goddard, JC. “The navy surgeon’s chest: surgical instruments of the Royal Navy during the Napoleonic War.” Journal of the Royal Society of Medicine, 97, (2004): 191–197; Croskery Howard, RP. “Surgery at Sea: An Analysis of Shipboard Medical Practitioners and Their Instrumentation.” MA Thesis, Department of History, East Carolina University, (2016), 25.
- Woodall, op. cit., 172.
- Sachs et al., op. cit.; Goddard, op. cit.
- Moyle, Chyrurgic Memoirs, 119. Cauterizing or vitriol buttons were pieces of caustic material that burned bleeding vessels closed.
- Cited by ltwilliammowett, 2022. “Beat to Quarters: Onboard Surgery.” https://ltwilliammowett.tumblr.com/post/680906138779287552/onboard-surgery [accessed December 29, 2023].
- Haire, L. “Remarks on Mr. Lucas’s Practical Observations on Amputation.” London Medical Journal, 7, (1786): 377–390.
- Dobson, J. “Nelson and the surgeons.” Journal of the Royal Naval Medical Service, 44, (1958): 111–117.
- Dionis, op. cit., 410 (references to an accompanying diagram omitted).
- e.g., Barlass, T. “The macabre history of surgery at sea.” The Sydney Morning Herald, February 5, 2016. https://www.smh.com.au/national/nsw/the-macabre-history-of-surgery-at-sea-20160203-gmkp0h.html [accessed December 29, 2023]; ltwilliammowett, 2020. “Beat to Quarters: The Sick Bay.” https://ltwilliammowett.tumblr.com/post/637237339037499392/the-surgeon-was-not-only-responsible-for-the [accessed December 29, 2023].
RICHARD DE GRIJS, PhD, is an astrophysicist and an award-winning historian of science at Macquarie University in Sydney, Australia. He has a keen interest in the history of maritime navigation. Richard is also a volunteer guide on Captain Cook’s H.M. Bark Endeavour replica at the Australian National Maritime Museum, where he additionally consults on aspects of the perennial “longitude problem.”