
JMS Pearce
Hull, England
{kind=link}
In my student days, the Wasserman reaction (WR), though not specific, was performed almost routinely in patients on medical wards to detect syphilis. Several direct and serological tests of varying sensitivity and specificity have now replaced the WR. Since reaching a historic low in 2000 and 2001, the incidence of syphilis has increased almost every year.1 In 2020, 133,945 cases of all stages of syphilis were reported in the US, and in the UK the rate of newly diagnosed cases in 2020 was twice that in 2012.2 A clinical diagnosis of syphilis is no longer the occasional curiosity it was at the end of the twentieth century, yet routine screening tests have fallen into disuse. Because we now have effective antibiotic treatment, both clinical clues and screening tests are of vital importance, especially in early and in asymptomatic latent cases.
Neurosyphilis
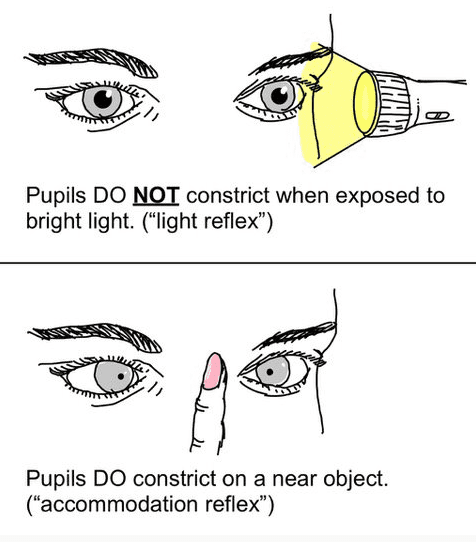
Historically, neurosyphilis was so common that Kinnier Wilson in his unique textbook Neurology in 1940 devoted over one hundred pages to it. Tertiary syphilis includes not only neurosyphilis but also gummata, cardiovascular, and meningovascular varieties.3 The Argyll Robertson (AR) pupil (Fig 1) is an important, classical sign of neurosyphilis.
Neurosyphilis may be asymptomatic with abnormal cerebrospinal fluid (CSF) but no neurological symptoms or signs. Symptomatic neurosyphilis most often presents with posterior column lesions, the hallmark of tabes dorsalis, typically fifteen to twenty-five years after primary infection. Argyll Robertson pupils are a valuable sign of tabes and may precede its typical sensory ataxia, absent ankle jerks, lighting pains, and visceral crises. General Paralysis of the Insane (GPI or dementia paralytica) presents with insidious and variable psychological symptoms, dementia, epilepsy, focal neurological deficits, and often AR pupils.3 Meningovascular involvement is caused by an inflammatory, obliterating endarteritis of the leptomeninges, brain, and spinal cord with resulting ischemic attacks or infarcts. About half the patients with neurosyphilis are infected with HIV.
Incidental neuroimaging abnormalities may also alert the neurologist to suspect neurosyphilis: cerebral gummata arising from the dura can mimic meningiomas, and medial temporal lobe abnormalities can mimic herpes encephalitis.
The Argyll Robertson pupil
Thanks to modern antibiotic treatment, the Argyll Robertson pupil (Fig 1) has become relatively rare. Unequal, irregular pupils without reaction to light had been known in cases of tabes dorsalis and dementia paralytica (GPI) since the end of the eighteenth century. In 1869, the ophthalmologist Douglas Moray Cooper Lamb Argyll Robertson (1837–1908) described his famous pupillary sign in two lengthy papers.
In the first, he reported the eye signs in a fifty-nine-year-old patient admitted on account of dimness of vision and an unsteady gait:4
In the second paper (1869), he reported four more cases and concluded the “myosis was due to paralysis of the cilio-spinal nerves,”5 although miosis is not a constant sign.6 Three of his cases had slight optic atrophy; one showed ptosis. Atropine drops produced only “medium dilatation of the pupils.”
Ernst Julius Remak had earlier shown the pupillary signs of tabes to Argyll Robertson,7 whose reports of 1869 acknowledged Remak’s observation of the miotic pupil, its defective reaction to light, and preserved contraction on accommodation. Argyll Robertson also cited Romberg’s Lehrbuch der Nervenkrankheiten des Menschen (1840): “In tabes dorsalis I have found the pupil contracted to the size of a pin’s head…one or both eyes, consisting in a contraction with loss of motion.”
The Argyll Robertson pupil soon became a “pathognomonic sign” in tabes dorsalis, dementia paralytica, and meningovascular syphilis. However, the role of syphilis in causing these disorders was at first debated, and not until the 20th century was it generally accepted.8 Crucial to this were the discoveries by Schaudinn and Hoffmann of the treponema pallidum in 1905 and the serologic test in 1906 of August Paul von Wassermann (1866–1925).
The abnormal pupil is probably caused by damage to cells in the pretectal region of the midbrain. As a result, signals carried from the retina are not relayed via the pretectal nucleus on the affected side to the Edinger-Westphal nuclei. This causes a loss of both the direct and consensual pupillary light reflexes. Since the accommodation reflex pathway is separate from the light reflex, it is unaffected. Unequal irregular pupils with iris atrophy and impaired reaction to light are the hallmarks, clinically distinguishable from the Holmes-Adie myotonic pupil. In an extensive review, Kinnier Wilson also reported AR pupils in cases of epidemic encephalitis and in tumors in the vicinity of the third ventricle and corpora quadrigemina, and rarely in disseminated sclerosis.6 It has also been observed in diabetic neuropathy, Wernicke’s encephalopathy, and Parinaud’s syndrome. By contrast, Sir Francis Walshe stated that “these components though varying from case to case are never found together apart from neuro-syphilis.”9
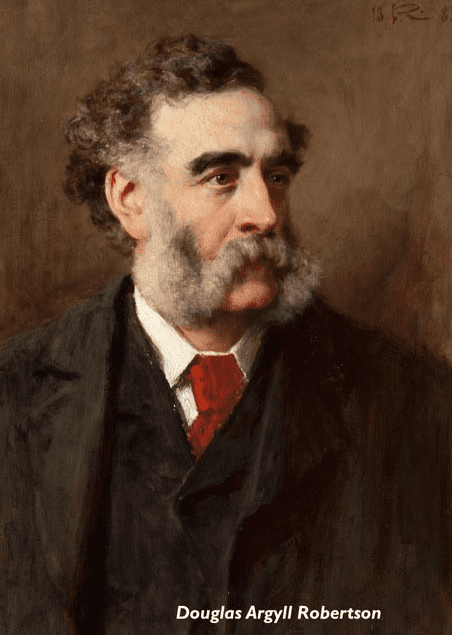
Argyll Robertson (1837–1909) was born in Edinburgh,10 where his father John was a general surgeon who specialised in eye surgery. He graduated from St. Andrews in 1857, returned to Edinburgh as a house surgeon at the Royal Infirmary, then studied in Berlin with the eminent Albrecht von Graefe before being appointed lecturer in eye diseases in Edinburgh in 1862.
A year later, he made his first significant discovery when into his own eye he instilled an extract of the Calabar bean (Physostigma venenosum), rich in the cholinesterase inhibitor physostigmine (syn. eserine). He noted: “it occasions contraction of the pupil, and sympathetically dilatation of the pupil of the other eye.” He rightly predicted it would become “most valuable in the ophthalmic pharmacopoeia.” It was and is still widely used in glaucoma, in which Argyll Robertson was also an early exponent of surgery.
In 1867, Argyll Robertson was appointed assistant ophthalmic surgeon, and in 1870 full ophthalmic surgeon to the Royal Infirmary, where he stayed until his retirement in 1897. In 1886, he was elected President of the Royal College of Surgeons of Edinburgh and was honorary eye physician to Queen Victoria and King Edward VII. In 1904 he moved to Jersey for health reasons. While on holiday in Gondal near Bombay in 1908, he became ill and died.
A biographer noted: “His handsome features and his tall, athletic frame made him the cynosure of all female eyes in his youth and in his later years, clad in a grey frock-coat and top hat, his dignified manner combined with his genial old-world courtesy made him conspicuous in any assembly and a magnificent ambassador of Scotland.” A talented golfer, he won the highly prized gold medal of the Royal and Ancient Club, St. Andrews five times.11
References
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2020. https://www.cdc.gov/std/statistics/2020/overview.htm.
- Nuffield Trust. Effectiveness of sexual health services. 2022. https://www.nuffieldtrust.org.uk/resource/effectiveness-of-sexual-health-services-1.
- Pearce JMS. Brain Disease Leading to Mental Illness: A Concept Initiated by the Discovery of General Paralysis of the Insane. Eur Neurol 2012; 67: 272-278.
- Argyll Robertson, DMCL. On an interesting series of eye symptoms in a case of spinal disease, with remarks on the action of belladonna on the iris. Edinburgh Medical Journal. 1869; 14: 696-708.
- Argyll Robertson DMCL. Four cases of spinal miosis: with remarks on the action of light on the pupil. Edinburgh Medical Journal, 1869, 15: 487-493.
- Wilson SAK. The Argyll Robertson pupil. In: Modern Problems In Neurology. London, Arnold 1928. pp. 332-358.
- Leake CD. Douglas Argyll Robertson. In: Webb Haymaker and Francis Schiller, eds. The Founders of Neurology. eds. 2nd edn. Springfield. Charles C Thomas 1970. p. 505.
- Pearce JMS. The Argyll Robertson pupil. J Neurol Neurosurg Psychiatry. 2004; 75(9): 1345.
- Walshe FMR. Diseases Of The Nervous System. Edinburgh, Livingstone, 10th edn 1963. p. 185.
- Obituary. Edinburgh Medical Journal, 1909; 3rd series, pp. 159-162.
- Bennett JDC. Argyll Robertson — a breadth of vision. Journal of Medical Biography, 1993, 1: 186–188.
JMS PEARCE is a retired neurologist and author with a particular interest in the history of medicine and science.