James L. Franklin
Chicago, Illinois, United states
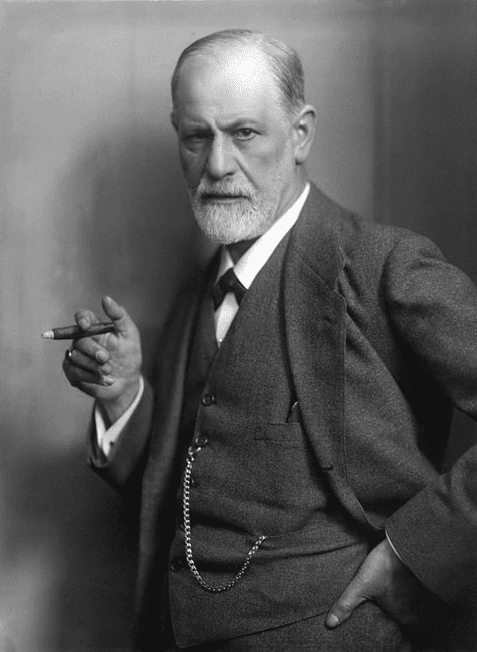
When the founder of psychoanalysis, Sigmund Freud, died in London early on the morning of September 23, 1939, he succumbed to what he wryly referred to as “my dear old cancer with which I have been sharing my existence for sixteen years.” Freud had been discovered to have carcinoma of the oral pharynx in 1923 at the age of sixty-seven. Given his fame at the time of his death and his importance in the fields of psychology and psychiatry, there exists extensive documentation of his life and work. Within the context of biographical studies, the facts about his medical history can be found in Ernest Jones’s (1879–1958) The Life and Work of Sigmund Freud or Peter Gay’s Freud: A Life for Our Time. A more focused account is found in Freud: Living and Dying written by Max Schur (1897–1969), Freud’s personal physician from 1929 until his death in 1939. Sharon Romm, a plastic surgeon and medical historian in The Unwelcome Intruder: Freud’s Struggle with Cancer presents an in-depth account of his doctors and the surgical procedures he endured. Numerous articles have appeared in medical specialty journals summarizing this history and commenting on technical aspects of his care. Freud’s own thoughts about his illness and care are scattered throughout his correspondence during the last decade of his life. A review of the illness and the care Freud received is of interest for the light it sheds on the practice of medicine during this era.1
When physicians become patients, they often resort to evasive strategies before accepting their illness. Freud was aware that he had a problem in his mouth in February of 1923 but hesitated to seek help until April of that year. He made light of the problem, recalling that during World War I, at a time when cigars were hard to come by, he had first noticed a painful swelling on his palate that receded when a patient presented him with a much-desired box of cigars. In a somewhat oblique manner, he showed the lesion to one of his friends, Maxim Steiner, a dermatologist and early member of the Viennese Psychoanalytic Society. Steiner told Freud it needed to be excised, calling it leukoplakia (a benign condition consisting of white patches on the mucous membrane). That evening when Felix Deutsch (1884–1964), a psychoanalytically oriented internist, visited Freud about other matters, Freud asked him to look at his mouth, cautioning: “Be prepared to see something you won’t like.”
Deutsch believed that the lesion was a cancer, but for a variety of reasons didn’t feel Freud could emotionally handle an explicit diagnosis and also called it leukoplakia. Deutsch urged Freud in a series of telephone conversations to seek an immediate surgical consultation. Freud decided to see Marcus Hajek (1861–1941), a professor of laryngology at the University of Vienna, although he expressed some reservations about Hajek to Deutsch, including the view that “no one should ask a friend for an operation on oneself.”2
Freud’s choice of Hajek came about indirectly through his friendship with Julius Schnitzler, a professor of surgery as well as Freud’s Saturday afternoon card partner. Schnitzler’s father, Professor Johann Schnitzler, was the founder of the Vienna Nose and Throat Clinic and Hajek’s father-in-law. The elder Schnitzler had initially opposed Hajek’s request to marry his daughter. Hajek had a dubious reputation as a surgeon, though he was a prolific author of scientific papers and textbooks. As a result of the marriage, Hajek’s career blossomed, and he eventually became the chief of the Rhinologic Hospital of the University of Vienna.
On April 20, 1923, Deutsch accompanied Freud to Hajek’s outpatient clinic, and the lesion was excised. Freud did not share knowledge of his surgery with his wife or daughter Anna, and Deutsch did not remain at the clinic with Freud during the surgery. The operation was complicated by a severe hemorrhage and was also flawed in that Hajek did not establish that the margins of the resection were free of tumor. Because of the bleeding, Freud was admitted to Hajek’s private hospital, but when no beds were available, he was relegated to a sort of closet room which he shared with a mentally disabled and deaf dwarf. His wife and daughter were summoned and they found Freud sitting in a chair in a dazed state, his gown covered with blood. His wife and daughter were persuaded to leave for lunch and returned to find that he had again hemorrhaged. He had been unable to call for help, and only through the efforts of his roommate was help summoned. After these events, Anna refused to leave her father alone. Accounts of this surgical misadventure also mention that when his condition seemed to deteriorate during the night, the clinic’s overnight physician refused to get out of bed to see Freud.3 Hajek paid little attention to Freud’s condition when he appeared in the morning, presenting his case to a group of students and arranging for his release from the hospital.
Ernest Jones, a Welsh neurologist and psychoanalyst, was Freud’s colleague, friend, and biographer, and characterized Hajek’s care as “cavalier.” Sharon Romm critiques Hajek’s management of Freud’s scar contracture, calling it “at least pitifully inadequate and at worst negligent.” Max Schur observed that “Freud was neither properly admitted to a ward nor transferred to the quite luxurious Löw Sanitorium, a private hospital one block away from the clinic.” He found his treatment inexcusable “even if the patient had not been someone who achieved world fame and was moreover, a friend of his brother-in-law’s [Julius Schnitzler].”
Jakob Erdheim (1874–1937), who was the Professor of Pathology at the University of Vienna, made a diagnosis of squamous cell carcinoma. Hajek advised radiotherapy, which was carried out by Guido Holzknecht, chairman of the radiology department. This treatment also included the use of radium capsules. By Schur’s account, the radiation caused tissue damage and violent pain. Schur was convinced that Freud was fully aware of the significance of radiation and radium treatment and deeply resented that he was not being told the truth.4
Hajek saw Freud several times after his surgery and allowed him to go on his usual three-month summer holiday with his family. Because of continued discomfort, Freud asked Deutsch to visit him while he was vacationing at Lavarone in northern Italy. Deutsch found a recurrence of the tumor and realized that further surgery would be required. He again did not share this information with Freud but discussed the matter with a small group of Freud’s intimate psychoanalytic colleagues, who were meeting nearby in the San Cristoforo in the Dolomites. Freud was profoundly indignant when he learned of this breach of patient confidentiality from Ernest Jones in 1938 after he had emigrated to London. With blazing eyes, he asked: “Mit welchem Recht?” (“With what right?”).
Deutsch allowed Freud to travel with his daughter and act as her guide to the ancient sites in Rome. The trip, one that he had dearly looking forward to making, was marred by an incident while on the train when he hemorrhaged profusely from the mouth. On his return to Vienna in September he was told the truth about his condition. Deutsch had arranged for him to see Professor Hans Pichler (1877–1949) who was chief of the Department of Oral Surgery. Deutsch left no clear indication how he came to select Pichler, but it was an ideal choice for Freud. Pichler would provide meticulous care for the next sixteen years, even traveling from Vienna to London in 1938 to perform the final of some thirty-three operations that Freud would undergo.

Hans Pichler was the son of a highly respected dentist who served the Austrian court. As a young man he was an outstanding athlete, first in all the classes at the gymnasium. He studied medicine at home in Vienna and also abroad in Fribourg and Prague. In 1900, he began his surgical career at the University of Vienna with distinguished surgeon Anton Eiselsberg. His career was upended when he developed eczema from the carbolic spray that surgeons used prior to surgery to disinfect their hands. His interest shifted to dentistry, and in 1902 he attended the Northwestern University Dental School in Chicago, studying under G. V. Black, who was considered “the father of modern dentistry.” On his return to Vienna, he embarked on a highly successful academic career and directed the Dental Institute of the University of Vienna. During World War I, he had operated on severely injured soldiers using heroic procedures that had never been attempted before, with excellent results.5 Pichler kept careful notes of every visit and surgery performed during the sixteen years he treated Freud. These were recorded using the Gabelsberger stenography system, then over 100 years old, that had been adapted to dental practice by his Pichler’s father. His medical record was left to Max Schur on Pichler’s death in 1949. Schur was able to persuade Pichler’s secretary, who could read his stenographic notes, to transcribe this important record of Freud’s treatment.6
Freud first visited Pichler on September 26, 1923 in his office located in a building on “Number 1” Lichtenfelgrasse, across from Rathaus Park. Pichler had already contacted Hajek prior to the visit, and on examining Freud, found a crater-shaped ulcer on the hard palate. The tonsillar pillars were shrunken and scarred from the previous excision, and the lymph glands beneath the lower right jaw were enlarged. Pichler explained the surgical procedure to Freud which would be performed in two stages and also require the fabrication of a prosthesis to preserve the integrity of the oral cavity. Freud faced this grim assessment with composure and a measure of humor. He related these events in a letter written on the same day to Max Eitingon (1881–1943), president of the Berlin Psychoanalytic Polyclinic, and refers to a “resurfacing” of “my dear neoplasm.”7
With characteristic thoroughness Pichler confirmed the feasibility of his surgical procedure on a cadaver. The operations were performed on October 4 and 11, 1923. In the first operation he ligated the external carotid artery and removed the lymph nodes beneath the right jaw. The second operation was designed to cure the cancer and involved removing part of the maxilla (upper jaw) and the mandible (lower jaw) on the right side as well as adding a skin graft to the inner lining of the cheek. This extensive surgery was performed with local anesthesia and opium sedation rather than general anesthesia. This approach was preferred so as to prevent the aspiration of blood.
During his first visit to Pichler’s office, Freud made it clear he did not wish to be treated as a colleague but charged as a private patient. The surgery took place in the operating theater at the Sanitorium Auersperg, a private hospital in suburban Vienna where paying patients were hospitalized. Those patients unable to pay a full surgical fee were treated at the Allgemeines Krankenhous. A photograph of the sanitorium built in 1907, as well as affirmation that Freud received kind and respectful care there, can be found in Sharon Romm’s The Unwelcome Intruder.
Freud’s post operative recovery was uneventful with only a single febrile episode, and by October 28, he was able to return home. Pichler saw his patient both at home and frequently at his office. On a return visit, excision of a necrotic skin tag yielded an unpleasant pathology report. On November 12, he was hospitalized, and a third operation was performed, requiring further removal of bone and another skin graft.
An integral part of Pichler’s surgical approach included the crafting of prosthetic devices to maintain the integrity of the oral cavity against contraction that would occur with healing. Pichler again was an ideal physician for Freud, combining his abilities as a surgeon and a dentist skilled in prosthetic construction.8 Hajek had given no attention to this issue during his initial surgery, and as a result trismus, a restriction of the range of motion of the jaw, was a prominent symptom when Freud was first seen by Pichler. As carefully as Pichler fabricated these devices, frequent adjustment was required and they were a constant source of discomfort. Freud referred to the prosthesis as “the monster.” After the third operation it was necessary that the prosthesis fit snugly to close an opening between the nasal and oral cavities.
A surprising sidebar in Freud’s medical history occurred on November 17, 1923. While convalescing from these three operations, Freud of his own volition underwent a Steinach operation, which was popular at the time. The operation was a vasectomy, a bilateral ligation of the vas deferens, in hopes that the resulting “rejuvenation” might delay the return of the cancer. The idea had been suggested to Freud by Rudolph Von Urban, a psychoanalyst who had worked with Eugen Steinach, the controversial endocrinologist who popularized the procedure.9
As a consequence of the surgical procedures of 1923, the quality of Freud’s speaking voice, which had been excellent, was never the same. The obturator prosthesis was necessary for him to be able to swallow but eating was a difficult affair and he avoided dining in public thereafter. Post-surgical infections involving the eustachian tube on the right side resulted in the unilateral loss of hearing, and a change in his famous consultation couch was necessary to position his good ear (his left) next to the head of the couch. Removal, replacement, and cleaning of the prosthesis were difficult tasks. Over the years, Freud became more and more dependent on his youngest daughter Anna’s nursing skills. There were instances when both Anna and Schur had to turn to Pichler for help. A special area next to Freud’s study was set aside with supplies, lighting, and equipment to manage this care.10
The struggle to find a suitable prosthesis led Freud to travel to Berlin in 1929 for a consultation with Hermann Schroeder, the director of the University of Berlin’s Dental Institute and its Division of Prosthetics. Freud had to remain in Berlin over a number of weeks. His loss of income during this time was such that when he received the Goethe Prize in 1930, the two-thousand-dollar prize money barely covered his expenses. In September 1931, the American plastic surgeon Varaztad Kazanjian was approached by Marie Bonaparte and Ruth Mack Brunswick at a surgical meeting in Berlin, where they asked him to come to Vienna and try to construct another prosthesis. Kazanjian, who was on the Harvard faculty, at first declined. Brunswick’s father, federal Judge Julian Mack, a member of Harvard’s Board of Overseers, was in Paris at the time and traveled to Berlin to persuade Kazanjian to see Freud in Vienna. The fittings were performed in Pichler’s office and in the end were no more satisfactory than those that Pichler had constructed. Kazanjian’s fee for the journey was $6000, which Freud could ill afford.
Marie Bonaparte (1882–1962) was the great-granddaughter of Napoleon Bonaparte’s brother Lucien Bonaparte. Through her marriage, she was also the princess of Greece and Denmark. She had been analyzed by Freud and became a lay analyst herself, contributing articles to the psychoanalytic literature. During the last decade of his life, Freud corresponded regularly with her and shared many of his thoughts about his illness. She played a vital role in protecting the Freud family in 1938 by contributing financially to secure their escape from Austria.
Inextricably woven into the fabric of Freud’s medical history was his addiction to cigars. This habit that he could not master and which mastered him played an undeniable role in the relentless course of his oral cancer. Portraits of Freud rarely find him without a cigar (his favorite brand was Don Pedro). He seems to have been in a state of denial as to the hazards of smoking. Freud’s nephew Harry recalled refusing a cigarette at the age of seventeen and his uncle telling him, “My boy, smoking is one of the greatest and cheapest enjoyments in life, and if you decide in advance not to smoke, I can only feel sorry for you.”
In 1923, at the time his cancer was diagnosed, he was smoking up to 20 cigars a day. His physicians repeatedly urged him to stop. Jakob Erdheim, a towering figure in the field of pathology in Austria and Germany, read the numerous biopsies taken during the course of Freud’s illness and repeatedly pointed out the relationship between tobacco and the precancerous and cancerous changes. Erdheim added to his report: “The patient should be strongly advised to give up smoking.” When Schur showed him such reports, Freud merely shrugged his shoulders.
Freud began smoking cigarettes at the age of twenty-four and soon switched exclusively to cigars. For Freud, smoking was essential to his capacity to work, a belief he expressed on many occasions. In an attempt to rationalize his dependence on tobacco he recalled that his father was a heavy smoker and remained one for his entire life living to the age of eighty-one. Only on one occasion had Freud succeeded in abstaining from tobacco for any significant period of time. In his late thirties, he suffered from a variety of cardiac symptoms including arrythmias and anginal complaints. His friend and colleague at the time, the internist Josef Breuer, believed his symptoms were the result of nicotine poisoning. Wilhelm Fleiss, a rhinologist who was to share his early psychoanalytic theories, persuaded him to stop smoking. Freud succeeded in this for a period of fourteen months.11 During these years, Freud experimented with cocaine to the point of addiction. Howard Markel has thoroughly reviewed the history of Freud’s use of cocaine, which included a number of months in 1899 when he became a bit too attached to wine. Markel suggests that if there is an “addictive personality,” Freud would qualify as an ideal candidate.12
Because Freud had lost confidence in Felix Deutsch due to his lack of candor in revealing the true nature of his oral cancer, he was without a personal physician after 1923. He relied on informal consultations with friends including Ludwig Braun, a cardiologist; Lajos Levy, an internist; and Oskar Rie, a friend of the family and his children’s pediatrician. In 1929, Marie Bonaparte convinced Freud to seek a personal doctor and recommended Max Schur. Marie Bonaparte had met Schur when she had been his patient seeing her through a serious illness. She was impressed with Schur as an internist and also for his embrace of psychoanalysis. As a student, Schur had attended Freud’s Introductory Lectures on Psychoanalysis on Saturday evenings in 1916 and 1917. He had also undergone personal analysis in 1924. Schur was somewhat apprehensive on his first meeting with Freud, fearing he would find him too young and inexperienced. Schur was thirty-one at the time, some forty years Freud’s junior. The meeting went very well and before telling Schur his medical history and present complaints, Freud made Schur promise he would always be told the truth and “that when the time comes, you won’t let me suffer unnecessarily.” As he had with Pichler, Freud ended their interview by insisting he did not wish to be given professional courtesy and wanted to be charged a normal fee. It was the customary at the time in Vienna for doctors to submit their bill at the end of the year. In January 1930 when Freud asked for Schur’s bill, he returned it as “inadequate” and reflecting an “unprofessional disregard of medical accomplishment.” He suggested that Schur send him a more appropriate statement. The role Schur assumed was referred to as a “Leibarzt.” This was a personal physician aware of their patient’s overall physical condition, a luxury that only a few could afford and perhaps equivalent today to a concierge doctor. It was a role Schur would faithfully fulfill for the remaining decade of Freud’s life.
In the summer of 1936, Schur “observed the rapid development of an ugly-looking lesion” in Freud’s mouth. Pichler took an initial biopsy which revealed malignant tissue. Freud was informed of the pathological findings. This was the first instance that malignancy had been found in thirteen years of careful surveillance and frequent biopsies. A more extensive operation was performed under general anesthesia using nitrous oxide. Then, early in 1938, Freud asked Pichler to remove “an old atheroma from under the left mandible because it had recently grown, bothering him when he attended to his beard, and because it looked ugly.” Again, the pathology report revealed cancerous tissue. Pichler was hesitant to tell Freud but Schur felt bound to inform him. As he had in 1936, Freud took the news with no sign of emotion.
Freud’s outlook on death and his own demise was complex. He could be droll citing George Bernard Shaw’s The Doctor’s Dilemma: “Don’t try to live forever since you won’t succeed,” and he could be resigned as when he wrote Marie Bonaparte, “with every illness new signs of the deterioration of old age push themselves forward.” He hoped to reach the age of his father and older brother who both lived into their early eighties.
The deterioration in the political situation in Austria and the Anschluss on March 11, 1938 was followed by a sequence of unpleasant events that convinced a reluctant Freud to accept the urgings of his friends that he go into exile. The details of his rescue from the Nazis in 1938 can be found in the Ernest Jones and Peter Gay biographies as well as a recent publication, Saving Freud, by Andrew Nagorski. Freud and his immediate family and household were able to leave Vienna on June 4, 1938 aboard the Orient Express. There were tense moments when the train crossed the border into France at 3:30 in the morning. Later that morning the train pulled into the Gare de l’Est in Paris. They all were chauffeured to Marie Bonaparte’s villa in St. Cloud where a luncheon was served while they rested until the evening when they crossed the channel to England by night ferry. Schur, who was to accompany the family as Freud’s Leibarzt, suffered an attack of acute appendicitis requiring an operation. It was arranged that Josephine Stross, a pediatrician and friend of Anna, would accompany Freud on the journey. While still convalescing from the operation, Schur and his family were able to leave Vienna about a week later. Schur observes that it was amazing “how well not only Freud but many very old people withstood journeys overseas at that time, frequently under most primitive conditions.”
Freud’s arrival in London on June 7, 1938 was enthusiastically reported in the British press. The Lancet pointed to the debt he was owed by psychologists and psychiatrists as well as pride in the fact that Britain could offer him asylum. These sentiments were echoed by the British Medical Journal. On June 23, officials from the Royal Society of Medicine, which two years earlier had made him an honorary fellow, called at his home so he could sign their charter book. Removing the charter from the offices of the Royal Society was made in deference to the status of his health, an exception normally reserved only for the King. Freud thus found himself in “good company” with Charles Darwin and Isaac Newton, other notable members of the Society.
Schur had been granted permission by the British Home Office to function officially as Freud’s physician before he had passed the required examinations. Pichler had recommended oral surgeon George G. Exner (1902–1965) and provided a letter with the details of Freud’s case. Exner was a South African who had studied plastic surgery in Berlin and with Pichler in Vienna. In July and August, Schur noted the appearance of suspicious new lesions in Freud’s oral cavity but felt that as a foreigner, Exner didn’t accept his concerns. In September, Schur contacted Pichler and persuaded him to see Freud in England. Pichler arrived in London on September 7, 1938 and found the lesion was of concern. On September 8, he performed a major operation under general anesthesia at a fashionable private hospital, the London Clinic. Freud tolerated the surgery well, and Pichler was able to return to Vienna the next day. News of the operation was extensively carried in the London press. When the pathology report revealed pre-cancerous tissue, Exner commented to Schur that perhaps the surgery had not been necessary. Given the political tensions at the time, it is remarkable that Pichler was able to travel to London and perform surgery in a foreign country.13
By September 27, 1938, Freud moved into his permanent London address at 20 Maresfield Gardens. The home and been purchased in July, and Freud’s son Ernest, an architect, attended to the remodeling, which included the instillation of a lift that could carry Freud to the second floor. Anna Freud and Marie Bonaparte arranged Freud’s study, including furniture and art objects as well as his famous couch, which had all come from Vienna and duplicated his old surroundings in Berggasse 19. Freud was able to resume seeing four patients a day and receiving visitors.
There was a gradual improvement in Freud’s health, but it did not last. Schur observed the appearance of a new lesion in January 1939. Again, Exner insisted that it was an inflammatory lesion. On February 10, Freud was seen by Wilfred Trotter (1872–1939), a Royal Society Fellow with expertise in surgery of the tongue, nasopharynx, and larynx. Trotter was also the brother-in-law of Ernest Jones and had helped Jones place the request to allow Freud to emigrate to England before the British home secretary. Neither Exner nor Trotter was convinced the lesion was significant. Schur sought help from Marie Bonaparte and a consultant from the Institut Curie in Paris, Dr. Lacassange, saw Freud in London and recommended a biopsy. This was performed at the end of February and the results again were cancerous. Further surgery was deemed impossible and a course of radiotherapy was begun at the office of an English radiologist, Dr. Finzi. The daily trips to his office were a great strain for Freud.
It was at this time Schur faced a difficult choice. He had intended to remain in London with Freud while he was alive and then emigrate to the United States. Visas were difficult to obtain and when they arrived for himself and his family, he was forced to go to New York and take his New York State Boards for his medical license. With great misgiving, Schur left for New York on April 21, 1939 and with help from Julian Mack was able to expedite the examination process, returning to London by July 9. He trained a physician friend, Dr. B. Samet, to fill in for him during his absence, but knew Freud was apprehensive over his departure.
On his return to London, Schur found Freud’s condition had significantly deteriorated. He had lost weight and was somewhat apathetic. He had lost his beard on the right side of his face as a result of the radiation treatment. The prior surgical site exuded a foul necrotic tissue and there appeared to be a new carcinomatous lesion higher in his mouth. From this point forward Freud’s condition was in steep decline. He had to give up seeing patients. His study was converted into a sickbay, and Schur moved into the house to help with his care. He was requiring around-the-clock nursing and frequent applications of Orthoform, a crystalline powder with a chemical structure similar to cocaine. Freud was unwilling to take any pain medication stronger than aspirin. Necrosis of the skin developed over his cheek and progressed to a full thickness opening into the oral cavity.14 All attempts at oral hygiene failed to suppress the foul odor such that even his beloved chow Lün shrunk from his presence, crouching in the farthest corner of the room.
From Schur we learn that the last book Freud read was Balzac’s La Peau de Chagrin (The Wild Ass’s Skin). The protagonist, Rapheal de Valentin, gains possession of a wild donkey’s skin and in a Faustian bargain with the Devil is granted all he wishes. Each time he makes a wish, the skin shrinks. Freud was very careful in his choice of books. On finishing the book, he told Schur, “This was the proper book for me to read: it deals with shrinking and starvation.”
Finally, on September 21, Schur recorded:
While I was sitting at his bedside Freud took my hand and said to me: “Leiber Schur. Sie ernnern sich wohl an unser erstes Gespaach. Sie haben mir damals versprochen mich nicht im Stiche zu lassen wenn es so weit ist. Das ist jetzt nur noch Quälerei und hat keinen Sinn mehr.” (My dear Schur, you certainly remember our first talk. You promised me the not to forsake me when the time comes. Now it’s nothing but torture and makes no sense anymore.)
Schur indicated he had not forgotten. Freud thanked him and requested he inform Anna. The next morning when Freud was in pain, Schur gave him an injection of “two centigrams” of morphine. The dose was repeated twelve hours later, and Freud lapsed into a coma, dying at 3:00 A.M. on September 23, 1939. It was the first day of Yom Kippur.
Since the published accounts of Freud’s final days appeared in the biographies of Ernest Jones and Max Schur, commentary has appeared on both the details of his final hours and the subject of physician-assisted suicide. Recollections provided by Paula Fichtl, a long-serving live-in-maid in the Freud household, and from Dr. Josephine Stross, the friend of Anna Freud, who accompanied Freud and his family when they left Vienna in 1938, suggest that Stross administered a third dose of morphine before Freud’s death and that Schur was not present at the time of death.15 Discrepancies in the details of Freud’s final hours have been analyzed in detail by Roy B. Lacoursiere in an article in American Imago. Jones and Schur may have wanted to protect Stross, who was still in practice, from the charge of euthanasia. In commentary by Jack D. McCue and Lewis M. Cohn that appeared in the Archives of Internal Medicine in 1999, the authors are unequivocal that Freud’s suffering and death was eased by assisted suicide. They praise the fact that Freud was able to rely on the sensitivity of his personal physician not to abandon him at the moment of death.16
Still, despite the controversial circumstances of his death, Freud’s determination in the face of his illness to continue to treat others is remarkable. Schur and Pichler stand out for the dedicated care they provided throughout his life, and Anna Freud gave her father both love and devotion as well as her dedication to preserve his legacy.
End notes
- Ernest Jones, The Life and Work of Sigmund Freud, Volume 3 – The Last Phase 1919-1939, New York Basic Books Publishers, 1957; Peter Gay, Freud: A Life for Our Time, W. W. Norton & Company, 1988; Max Schur, Freud: Living and Dying, International Universities Press, Inc. 1972. Sharon Romm, The Unwelcome Intruder: Freud’s Struggle with Cancer, Praeger Publishers, 1983.
- Felix Deutsch, Reflections on Freud’s One Hundredth Birthday, Psychosomatic Medicine, 1956, 8 (4): 279-283.
- Nicholas Lazaridas, Sigmund Freud’s oral cancer, British Journal of Oral and Maxillofacial Surgery (2003) 41, 78-83. Similar accounts of Freud’s first operation can be found in the biographical sources in footnote #1.
- Max Schur, Freud: Living and Dying. Chapter 13, “1923 – The Cancer Surgery” may be consulted for an in-depth discussion of Freud’s attitudes about the cancer diagnosis and his physician’s reluctance to reveal the diagnosis.
- Schur, Freud: Living and Dying, p. 361.
- A useful English abstract of these notes can be found in the third volume of Ernest Jones’s The Life and Work of Sigmund Freud, Appendix B.
- “My dear neoplasm has reappeared” appears in Freud’s letter in German, “da das liebe Neugebilde dort aufgetaucht ist.”
- Romm, The Unwelcome Intruder, Chapter 9, “The Prosthesis” provides an overview of the materials and techniques used in prosthetic fabrication at the time of Freud’s surgery and specific information of the prostheses that were made for him.
- For a historical discussion of Medical Rejuvenation see: James L. Franklin, Rejuvenation, “The Adventure of the Creeping Man” from The Case-Book of Sherlock Holmes, Hektoen International, https://hekint.org/2021/10/14/rejuvenation-the-adventure-of-the-creeping-man-from-the-case-book-of-sherlock-holmes/ and John B. Nanninga, The Gland Illusion: Early Attempts at Rejuvenation through Male Hormone Therapy, McFarland & Company, Inc., Publishers, 2017.
- A photograph of the “treatment area” can be found on Plate 19 in Berggasse 19: Sigmund Freud’s Home and Offices, Vienna 1938, The Photographs of Edmund Engelman, The University of Chicago Press, 1976. Photographs of Freud’s Prostheses can be found in John C. Davenport, Sigmund Freud’s Illness—The Ultimate Team Approach to Head and Neck Cancer, Facial Plastic Surgery, (1993), 9(2): 125-132.
- Schur, Freud: Living and Dying, Chapter 2 – “Freud’s Cardiac Episode: The Battle Against Nicotine Addiction” contains a thorough discussion of Freud’s cardiac symptoms and attitudes toward smoking.
- Howard Markel, Anatomy of Addiction: Sigmund Freud, William Halsted, and the Miracle Drug COCAINE, Vintage Books, 2011, p. 31.
- Mark Edmundson, The Death of Sigmund Freud: The Legacy of His Last Days, Bloomsbury, 2007. See pages 196-197. Anton Sauerwald, a controversial figure and German officer who had been overseeing the Freud family, became sympathetic to their cause. He aided their escape to London by hiding the fact that Freud illegally sent money abroad. He visited London in October 1939 and claimed to have had a role in arranging Pichler’s visit to London. See Murray G. Hall, “The Rise of the Internationaler Pyschoannalytischer Verlag,” in Freud in Exile, edited by Edward Timms and Naomi Segal, Yale University Press, 1988.
- Romm’s The Unwelcome Intruder provides a history of orthoform in dental practice and mentions tissue necrosis as a potential adverse effect (p. 92-93). Could Freud’s long usage of this substance have been a factor in the necrosis of his cheek? Most sources suggest that the cancer caused the gangrenous necrosis of his cheek. Freud received X-ray treatment and radium treatments on numerous occasions. Dosage was not standardized and one wonders if a cumulative overdosage played a role in the necrosis of his right cheek.
- Alastair D. Macleod, Was Sigmund Freud’s death hastened? Internal Medicine Journal (2017) 47:966-969 and Roy B. Lacoursiere, Freud’s Death: Historical Truth and Biographical Fictions, American Imago (2008) 65 (1): 107-128.
- Jack D. McCue and Lewis M. Cohen, Freud’s Physician-Assisted Suicide, Archives of Internal Medicine, (1999), 159: 1521-1525.
JAMES L. FRANKLIN is a gastroenterologist and associate professor emeritus at Rush University Medical Center. He also serves on the editorial board of Hektoen International and as the president of Hektoen’s Society of Medical History & Humanities.