
JMS Pearce
Hull, England
Aphorisms from wise medical men and women have fallen out of fashion. Because each line is to a degree debatable, one of my favorites is:
Attitudes are more important than abilities.
Motives are more important than methods.
Character is more important than cleverness.
Perseverance is more important than power.
And the heart takes precedence over the head.
Its author was Denis Burkitt, who often used it when asked to autograph a book or paper. It could with benefit be placed on the desktop of every doctor and aspiring medical student.
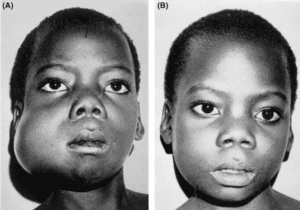
Burkitt had the distinction of discovering a new type of childhood cancer in unusual circumstances. In 1957 Hugh Trowell, a physician at Mulago Hospital in Uganda, asked his colleague Denis Burkitt to examine a five-year-old boy with swellings on both sides of his upper and lower jaws. Burkitt had seen children with jaw tumors before, but it was the first time he had seen multiple symmetrical ones. Shortly afterwards he saw a girl with identical jaw swellings. At first, the biopsy pathology was inconclusive. Burkitt was puzzled. He realized he had stumbled across something new and sought more such patients,1,2 commenting, “A curiosity can occur once, but two cases indicated more than a curiosity.” His searches found forty-one children presenting with jaw tumors.3 (Fig 1)
Histology was available in twenty-nine of these, which disclosed a malignant lymphoma with massive proliferation of large, primitive cells of lymphoreticular tissue and pronounced phagocytosis.
Showing his ingenuity, he then studied the hospital’s records of all childhood cancers; he found that jaw tumors were often associated with other unusual tumors of the ovaries (bilateral), thyroid, salivary glands, adrenals, testes, spinal extra-dural space, and the orbit, excluding the eye. Most children perished within four months.
Burkitt realized that these were part of an unrecognized tumor complex that was common in Uganda. Subsequent pathological studies4 confirmed this and established a new type of B-cell, “Burkitt’s lymphoma,” common in Africa.
Burkitt traveled extensively (on a two hundred and fifty pounds grant) to trace its geographical distribution and found the prevalence of lymphoma was related to local temperature and rainfall. With Greg O’Conor he presented the preliminary epidemiology.1,5 This suggested to his colleague Anthony Epstein a cancer virus transmitted by an arthropod-borne agent.6 After two years working with tumor cells from Burkitt’s patients, Epstein discovered the Epstein-Barr virus (EBV) in Burkitt’s lymphoma cells in 1964.7 EBV infection is present in nearly all endemic African cases but in only a minority of sporadic (non-African) cases. Burkitt’s lymphoma is categorized into three subtypes: endemic, sporadic, and immunodeficiency-associated, each with unique clinical and pathological characteristics and response to treatment. (In 90% of cases the pathogenesis has subsequently been characterized by chromosomal translocation, which juxtaposes the c-MYC oncogene on chromosome 8.8)
In the 1960s, Burkitt obtained supplies of the drugs methotrexate, cyclophosphamide, and vincristine. Even in low doses they produced dramatic remissions or regressions of the tumors. In present-day Africa, Burkitt’s lymphoma accounts for many childhood malignancies, but many sporadic and adult forms with a worse prognosis have been recognized elsewhere. DA-EPOCH (dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) is the current primary treatment.
Burkitt’s discoveries initiated extensive new research in this field that led to the more general conclusion that viruses are involved in the etiology not only of Burkitt’s lymphoma, but of nasopharyngeal carcinoma, human T-cell leukemia virus type I, hepatitis B virus in hepatocellular carcinoma, and human papilloma virus in cervical carcinoma.6,7
When he returned to England, he was appointed to the MRC External Scientific Staff and Honorary Senior Research Fellow at St. Thomas’s Hospital. New investigations with Surgeon-Captain T.L. Cleave RN and H.C. Trowell convinced him of the role of a low-fiber diet in causing colonic diverticular disease, diabetes, hemorrhoids, deep vein thrombosis, and bowel cancer. These disorders had a much lower prevalence in Africans, who ate a high-fiber diet as compared with the low fiber diet of Western countries.9,10 This idea, though perhaps overstated by Burkitt, remains feasible but unproven; no definite link with bowel cancer has been identified.
Denis Parsons Burkitt MD, FRCS (Ed), FRS

Denis Burkitt (1911–1993) was born near Enniskillen, County Fermanagh, Northern Ireland, the son of James, an engineer. His family were devout Presbyterians and his religion was always important to him.
As a boy he attended Portora Royal School in Enniskillen, where both Oscar Wilde and Samuel Beckett had been pupils; he later moved to Dean Close School in Cheltenham, a stronghold of evangelism. He studied engineering at Trinity College, Dublin, but did not do well; he soon found his calling to become a missionary and therefore switched to medicine.11 He graduated near the top of his class in 1935 and then trained in surgery, acquiring the FRCSEd in 1938.
In 1940 he volunteered for the Royal Army Medical Corps (RAMC) but was rejected. He failed applications for work abroad, but on reapplication found employment as a RAMC doctor. He married Olive Rogers, a ward sister who shared his religious beliefs, in July 1943. They had three daughters. A few months later, he embarked with his unit on a troopship for Mombasa. Burkitt served first with African troops in Kenya and Somaliland. Following demobilization in 1946, he joined the Colonial Medical Service and was sent to a 100-bed bush hospital to start a new service in Lira, which he described as the work of “a simple bush surgeon.” He was then moved to Mulago Hospital Uganda, where he made his seminal discovery; he remained there until 1964.
Burkitt was a cheerful, modest man who denied any suggestion of scientific scholarship. He was an enthusiastic lecturer, generous in giving acknowledgement to others.
Sir Anthony Epstein FRS and MA Eastwood aptly described him:
Denis was a kind man possessed of wit and insight. He was proud that he had never spent a day in the laboratory and had always worked as an epidemiologist. He often spoke of the importance of simple observational studies and contrasted these with ‘the limitations of modern medicine’. But it was his unshakeable faith in the divine ordering of everything in life that inspired his observations.6
He was president of the Christian Medical Fellowship and lectured and wrote frequently on religious and medical themes. In 1979 he became an honorary fellow of Trinity College Dublin. He received numerous prizes and honorary doctorates. In 1970 he was made a Companion of the Order of St. Michael and St. George (CMG), and in 1972 a Fellow of the Royal Society. He died of a stroke on 23 March 1993 and was buried in Bisley, Gloucestershire.
References
- Burkitt D. A Sarcoma involving the jaws in African children. British Journal of Surgery 1958; 46 (197): 218–223.
- Burkitt DP, Wright, DH. (eds) (1970) Burkitt’s lymphoma, pp. 1-251. Edinburgh. Livingstone.
- Coakley D. (2006), Denis Burkitt and his contribution to haematology/oncology. British Journal of Haematology, 135: 17-25.
- O’Conor GT. Malignant Lymphoma in African Children, Part 2: A Pathological Entity. Cancer 1961;14, 270.
- Burkitt D, O’Conor GT. Malignant lymphoma in African children—A clinical syndrome. Cancer 1961;14:258-264.
- Denis Parsons Burkitt. 28 February 1911-23 March 1993. Biographical Memoirs of Fellows of the Royal Society Vol. 41 (Nov 1995), pp. 88-102. https://royalsocietypublishing.org/doi/pdf/10.1098/rsbm.1995.0006
- Epstein, MA, Achong BG, Barr YM. Virus particles in cultured lymphoblasts from Burkitt’s lymphoma. Lancet 1964;1: 702–703.
- Taub R, Kirsch I, Morton C, Lenoir G, Swan D, Tronick S, Aaronson S, Leder P. Translocation of the c-myc gene into the immunoglobulin heavy chain locus in human Burkitt lymphoma and murine plasmacytoma cells. Proc Natl Acad Sci 1982;79: 7837–7841
- Burkitt DP. Epidemiology of cancer of the colon and rectum. Cancer 1971;28(1):3–13
- Burkitt DP. Some diseases characteristic of modern Western civilization. Brit Med J 1973;1:274-278
- Burkitt DP. Direction Determines Destination. Christian Medical Fellowship. Nucleus April 1993. https://www.cmf.org.uk/resources/publications/content/?context=article&id=444
JMS PEARCE is a retired neurologist and author with a particular interest in the history of medicine and science.