Mark Tan
Northwest Deanery, England, United Kingdom
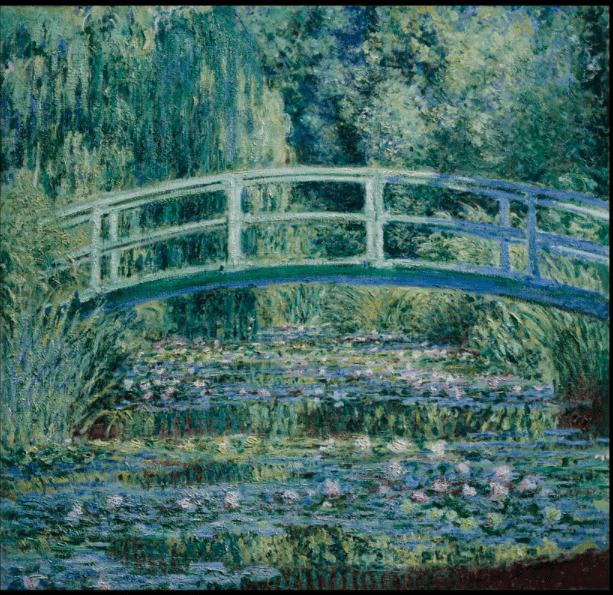
#/media/File:Claude_Monet_-_Water_Lilies_and_Japanese_Bridge_-_Google_Art_Project.jpg){kind=link}
“[Monet was] only an eye – yet what an eye.”
— Paul Cézanne
Much has been written about Claude Monet’s ophthalmic pathology.1-4 However, attributing his stylistic development to cataracts alone seems an overly reductionist view. In 1874, at least fifteen years before his Japanese Bridge and Water Lilies series, his painting Impression, Sunrise drew scathing criticism from art critic Louis Leroy, who described it as a partially finished wallpaper5 and in essence unwittingly coined the Impressionist movement. Contrary to Leroy’s criticisms, Monet had purposefully diverged from the widely accepted practice of idealizing a scene. He considered light and its effect on colors, and movement and its effect on visual perception. He began painting outdoor scenes and would paint with wet paint over wet paint, dramatically widening the range of contrasts, textures, and depths he could achieve. Central to the Impressionist philosophy was the artist’s own perception of the scene, which included the influence of environmental conditions, lighting, and his own emotions.6,7 This progression from a focus on exquisite detail to one of experiential complexity paralleled my own training in intensive care medicine and the journeys of some of my patients.
In medical school, I was obsessed with details. Fascinated by the intricacies of the human body, I looked up each syndrome, learned each blood test, and memorized the finer details of anatomy. From Asperger’s and Alport syndromes to Z-lines and ZAP70, the study of medicine seemed clear cut. If only one knew all the labels, pathways, and interactions, medicine could be mastered. A particular multi-system disease like sickle-cell anemia may present with signs and symptoms such as severe abdominal or bone pain, shortness of breath, and heart failure. It may be suspected by anemia, and then confirmed through blood film. The sickle shape of red blood cells, the result of misfolded hemoglobin protein caused by a single amino acid substitution, explained the multisystemic manifestations.8 It was logical, linear, and lucid.
This reductionistic approach to the study of medicine was both empowering and suppressive. Breaking down the unfathomable complexity of the human body into fundamental constituents seems to empower mere mortals to push the frontiers of scientific understanding. Linnaeus’ taxonomical hierarchy provided a structure with which to distinguish morphological differences between species, genus, and family.9 Watson and Crick’s discovery of the building blocks of DNA has formed the basis for the entire field of genetic medicine.10 Yet at times this seemingly universal philosophy within science fails to consider the entirety of human experience. The complexity of human pathology, irrationality of human behavior, and the unpredictability of critical illness defy the rigid attempts of reductionism to classify and categorize. Medicine, if practiced with a purely reductionist approach, would indeed be suppressive, going against the Hippocratic oath to “do no harm or injustice [to patients].”
As I progressed through specialty training, I began to learn more about the inadequacies of the reductionist thought process. The exact concentration of C-reactive protein (CRP) in the blood was not as useful as learning to develop an overarching impression of clinical trajectory. Taken in isolation, a single blood test may contain false positives, false negatives, time lags, or various interactions, all of which makes it impossible to correlate a test with what really matters to a patient: health and well-being. Experienced clinicians have learned such acumen and are able to collate and process information from the history, examination, and investigation modalities, so as to formulate an impression from otherwise disparate data. I learned likewise. Instead of trying to correct every test result to normality, I found my perception changing. I started looking at patients and their quality of life, instead of merely whether they would live or die. I explored their priorities, their social networks, and their spiritual needs. Taking these into account allowed me to build a fuller, richer, and more holistic clinical picture, one that would enable me to make better and more humane decisions. This was the art of medicine. The clinical examinations were my brushes, investigations were my paints, and the history became my scene, environment, and lighting. I became an impressionist. A couple of years ago though, I realized that this learned approach was confined neither to artist nor physician.
Gurjit was a frail, elderly gentleman who had several co-morbidities limiting his daily function. When he developed severe pneumonia, he was intubated and ventilated. One by one his organs started to fail. We were already pessimistic about his prognosis, so I spoke to his son Billal on the phone to voice my concerns about his father’s critical condition.

#/media/File:Claude_Monet_-_The_Japanese_Bridge_-_61.36.15_-_Minneapolis_Institute_of_Arts.jpg){kind=link}
“What are his saturations?” Billal asked.
“Ninety-four percent, but he needs high levels of oxygen to keep that it at that level. Do you work in healthcare?” I asked.
“I’m a biochemist. I live overseas, but I’m also the only family Dad has.”
“Well, he is critically ill from a severe chest infection. As such, he has a significant chance of dying.”
“What are his CRP and white cell count?”
“They were fairly high but we shall see if the antibiotics help for now.”
I could not help but feel that Billal had failed to grasp the gravity of his father’s predicament. A few days later, Gurjit continued to deteriorate.
“But his saturations are now 95%. His CRP and white cell count are coming down. How can he be deteriorating?” came an unbelieving voice through the phone.
It seemed Billal was unable to comprehend the fact that his father was not making clinical progress. Mildly frustrated, I persevered with explaining that although his saturations were better, he needed more oxygen. While the inflammatory markers were marginally better, other organs were beginning to show signs of deterioration. Within a couple of days, Gurjit’s kidneys failed. Then his liver packed in. This was going to be a terminal event. It was unanimously decided that Gurjit was dying, and our priorities needed to shift toward palliation.
I called Billal again. Again, the telephone conversation began with questions about blood results and observations. Without the visual and environmental input of a physical visit to the ICU, Billal struggled to picture his critically ill father. Over the telephone, an overwhelming sensory experience had been diminished, dampened, and dulled. Several iterations later, it finally dawned on Billal that his father was indeed dying. The most sophisticated technologies were unable to save him. Then the questions began to change. Instead of focusing on minute details, Billal was able to form an impression of the situation. In Monet-like fashion, he started to develop an overall impression of his dying father, building up his mental image of illness and death. In similar fashion, I guided Billal in assimilating the clinical data we had collected over the last few days, encouraging him to form an overall impression of his deteriorating father.
“I will fly in tomorrow to see him, but I’m not sure what to expect. I’ve never been to an ICU before,” Billal said.
I painted a picture of an ICU over the phone, an overall impression a la Monet. Broad strokes of the environment, from the machines to the monitors. I filled in the muted colors; lines that were inserted into Billal’s father. Then the lights and shadows; the various beeps and alarms he might see and hear, the decisions to be made and the journey to death. I told Billal that a staff member would be with him, guiding him, much as I had prepared him for his visit.
The next day, as Billal stood in front of his dying father, his mind painted one last scene. Gone was the focus on vital signs. No longer were the intricacies of blood results important. Just like Monet’s impressions of the Japanese Bridge faded with his advancing age and deteriorating health, Billal’s last impression of his father was now filled with a more irregular palette, darker hues, blurred lines, and patchy reflections. The fatherly constant in Billal’s life was now merely a fleeting frame of a bridge. Comfortable, assuaged, and in no distress, I was now confident that Gurjit would die with dignity. This, I hoped, at the very least would form an equally beautiful final impression.
“Like a bridge over troubled waters, I will lay me down . . .” — Simon and Garfunkel
References
- Hajar R. Monet and Cataracts. Heart Views. 2016;17(1):40-41.
- Gruener A. The effect of cataracts and cataract surgery on Claude Monet. Br J Gen Pract. 2015;65(634):254-255.
- Kopplin P. Monet and his cataracts. Hektoen International. 2016;9(1).
- Metzler S. Monet’s illnesses: beyond cataracts. Hektoen International. 2020;13(1).
- Prodger M. The man who made Monet: how impressionism was saved from obscurity. The Guardian. https://www.theguardian.com/artanddesign/2015/feb/21/the-man-who-made-monet-how-impressionism-was-saved-from-obscurity. Published 2015. Accessed Jul 2021.
- Goetz A, Sander E. Monet at Giverny. Gourcuff Gradenigo; 2015.
- Tate. Impressionism. Tate Gallery. https://www.tate.org.uk/art/art-terms/i/impressionism. Published 2021. Accessed.
- Wilson M, Forsyth P, Whiteside J. Haemoglobinopathy and sickle cell disease. Continuing Education in Anaesthesia Critical Care & Pain. 2010;10(1):24-28.
- Paterlini M. There shall be order. The legacy of Linnaeus in the age of molecular biology. EMBO Rep. 2007;8(9):814-816.
- Pray L. Discovery of DNA Structure and Function: Watson and Crick. Nature Education. 2008;1(1):100.
MARK ZY TAN is an Intensive Care Medicine and Anesthetics junior doctor in Northwest England. He is writing a book of patient narratives exploring clinical, ethical, and moral dilemmas in ICU, framed within artistic and historical contexts. His Telephone Lament for Coronavirus and Lent Talk Letter to Lydia were both heard by over 1.5 million listeners on BBC Radio 4. His professional interests include point-of-care ultrasound and global health. Mark lives with his wife and two daughters. Their free time is spent tending to the garden, growing vegetables and mushrooms, rearing chickens, and keeping honeybees, although not always in that order.
Highlighted in Frontispiece Volume 13, Special Issue– Fall 2021