
Tony Ryan
Cork, Ireland
Introduction
Henry MacNaughton Jones (1844-1918) was born in Cork City and graduated MD at Queen’s College, Cork, in 1864. Just four years later he founded the thirty-bed Cork Ophthalmic and Aural Hospital, where he practiced as a physician and surgeon. In the first eleven years, the hospital treated over 2,000 inpatients and 20,000 outpatients.1 His book, Atlas of the Diseases of the Membrana Tympani, was published in 18782 and was his treatise on the diagnosis and management of aural afflictions. It was illustrated with fifty-four chromolithograph plates based on detailed color illustrations by Margaret Boole, the second of five talented daughters of Mary Everest and George Boole, the Foundation Professor of Mathematics at Queens University College, Cork.3
The atlas gives an interesting perspective on the practice of otology in Cork City (pop. ~80,000) during the late Victorian years. Like any good physician-author, MacNaughton Jones begins with a description of the normal ear before proceeding to describe aural pathophysiology. He presents diseases of the middle ear in both adults and children, many of which have been eradicated or mitigated to the extent that they are no longer commonly seen today. He then describes the medical and surgical interventions he used for treating these various conditions, which are summarized in the table below. But first, in the holistic management of aural conditions, MacNaughton Jones directs our attention to the general health of the otological patient, exemplified by encouraging “a change of air, tonics, cod-liver oil, and iron with quinine.”
| Conditions | Clinical Commentary | Treatments |
| 1. The normal membrana tympani | Normal anatomy, color (pearl to neutral grey), mobility on inflation, and absent of pulsation, rupture or perforation. | None required |
| 2. Exostosis in the meatus (osteoma) | These tumors frequently occur without any assignable cause. | “Nitrate of silver, chromic acid, and chloride of zinc, syringing with alkaline solutions, injections of iodide of potassium or hydrochlorate of ammonia.” Dentist drill. Sea-tangle (seaweed). camel hair pencil. |
| 3. Perforation of the membrana tympani | Often neglected in children. | Warm washouts. Astringents. Equal parts alcohol and glycerine. Leeches. Warm fomentation (never poultices). Artificial membranes (not specified). Tonsillectomy (by tonsil guillotine). Vesiculation fluid over the mastoid. |
| 4. Inflammation of the membrana tympani | Free depletion by leeches (“the artificial leech, if it can be had”). Warm fomentations. Vesiculation fluid over mastoid. Syphon douche to throat. Incision of the membrane if bulging. | |
| 5. Furuncles or abscesses in the external meatus | “. . . affects persons of all kinds of constitution . . . and at all ages. Occasionally these attacks are attended with alarming constitutional symptoms. As abscesses are particularly likely to recur, it is well to warn the patient of this tendency . . .” | Depletion with leeches (two to four). Constant fomentations (chamomile and poppies) using Maw’s aural douche. Warm injections of strained poppy water. Vesiculation of the mastoid skin helps allay pain, occasionally subcutaneous morphine is needed. When abscess has formed, surgical evacuation of the pus. Careful follow-up to avoid blockage of the meatus or recurrence of abscess. |
| 6. Vascular polypi | Removal of these troublesome growths is only the first step in the process of cure, as they may recur. | Use the rectangular ring forceps or the lever ring forceps of Toynbee to remove. |
| 7. The fibrogelatinous polypus | “The characteristic symptoms are deafness with catarrhal discharge occasionally mingled with blood.” | Removed using Wilde’s snare, a small polypus forceps or miniature vulsellum. |
| 8. Sebaceous tumor in cavity of the tympanum | Rare. “I had never before seen a case of this nature . . .” | Incision and removal. |
| 9. Membrane after removal of cerumen | “The usual complaint made by patients suffering from wax in the ear is a deafness, with a stupid feel, and some form of tinnitus. . . . The impaction of wax on the drum is usually caused by such imprudent practices as the insertion of rolls of paper, the corners of towels etc., into the meatus for cleansing purposes, and is often complicated by the wearing of cotton wool in the ear.” | Insufflate the tympanum after removal of the wax. |
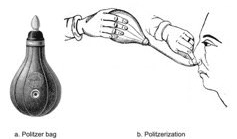
| 10. Eustachian obstruction and closure | “The malleus appears foreshortened, and the membrane has a tense stretched look, like a drawn curtain, often falling into similar folds. I have never seen a case of foreign body (except snuff) blocking up the tube.” | Blocked Eustachian tube should be inflated by Politzer’s bag, a hand-held rubber bulb with a narrow tip, used to infuse air or warm fluids. |
| 11. Collapse and rigidity of the membrane | “Suction of the meatus, as recommended by Hinton, I have frequently found of service in these collapsed state of the membrane. But it is a good plan to give a patient a piece of tubing with a quill inserted in one end to fit the meatus, and instruct him to apply suction with the mouth through the other.” | |
| 12. Catarrh of the tympanum, with brain complications | A case report of a little girl attending the hospital with aural catarrh and a bulging tympanic membrane. | “The child was to have been operated on the following day, but friends neglected to bring her. I afterwards learned that she died comatose and with convulsions. This is one of those cases where close attention to the ear and incision of the membrane may have saved life.” |
| 13. Hereditary syphilitic deafness | Poor outcome, invariably deaf. “I believe it is impossible to define any typical appearance in this affection, in which, I regret to say, that treatment has with me proved of little avail.” | “If taken in the first stages . . . mercurial treatment (inunction i.e. applied to the skin) followed by iodide of potassium internally at the same time that the Eustachian tube is attended to and the tympanic membrane kept free by warm iodide of potassium injections.” |
| 14. Cretaceous deposits of the membrane | “White layers of chalky substance on the membrane. . . . They may exist without much disturbance of the hearing . . .” | “I do not interfere” |
| 15. Inveterate eczema of the auricle | Particularly liable to recur. “. . . often loss of substance of the auricle with perhaps permanent disfigurement.” | Removal of scab, cleansing, chromic acid or carbolic acid. Chloride of zinc when scab is gone. Carbolized zinc and petroleum jelly at night. Meatus cleaned with forceps and syringing with chloride of zinc with glycerine and rectified spirit. Silver of nitrate to keep auricle healthy. |
| 16. Inflammation of the mastoid cells | Usually left with residual deafness. | Incision and drainage, debridement of dead bone, syringe with chloride of zinc, Dress with carbolic wool soaked in chloride of zinc |
| 17. External ear otohematoma (sanguineous tumor of the external auricle) | “Otohematoma occurs, with very rare exceptions, only amongst those affected with cerebro-mental disturbances. It was believed to be due to violence inflicted on the organ . . . but pathologists now look upon the affection as connected with the cerebral disorder and dependant probably on some intimate change in the cervical sympathetic nerves governing the vascular supply.” | Evacuation of blood and compression. “However, this is not usually possible in those with cerebro-mental disturbances.” |
| Table: Diseases of the ear as reported in the Atlas, including selected clinical commentaries in direct quotations and procedures performed by MacNaughton Jones. | ||
Condition 2. Osteoma: MacNaughton Jones reported that exostosis, a calcified mass obstructing the ear canal, was not uncommon in his practice. He describes these tumors as having no assignable cause. William Dalby some years earlier had made the observation that in a large proportion of cases the patient had been “addicted to sea bathing.”4 In addition to the chemicals noted in the table, other treatments included “a drill, similar to that used by dentists, has been employed to bore through the exostosis (Lancet, July 20, 1878) and sea tangle (brown seaweeds with fluted leathery fronds) subsequently employed to dilate the passage. Electrolysis has been employed with success. The aural probe is the most useful for cleansing the chink and applying solutions.” Subsequently, the patient needed to be involved in self-care in order to keep the ear canal patent: “A camel’s hair pencil, cut as to leave only a few central hairs, answers admirably for the patient to use himself.”
Conditions 3, 4, 5, 12. Suppurative disease: MacNaughton Jones was very concerned that children presented late in the course of illness, often with a perforated, discharging eardrum (aural catarrh). “Aural catarrh, acute or chronic, is often, shamefully, neglected in children: the younger the child and therefore the less competent to make its complaint known, the greater the probability of neglect.” Tragically, he described delayed or missed diagnoses in a number of children with suppurative disease who presented and subsequently died of “brain mischief” and cautions that, as every doctor is taught: “. . . aural mischief is, in a very young child, often masked by symptoms which direct attention away to other parts, the brain, the stomach, the teeth.” Suppuration in the tympanic cavity and mastoid cells have long been known to cause death through brain abscess, inflammation of the membranes covering the brain, or by pus entering the circulation from the lateral sinus.
Conditions 9, 10. Blocked eustachian tube: MacNaughton Jones recommended that a blocked eustachian tube should be inflated by Politzer’s bag, a hand-held rubber bulb with a narrow tip used to infuse air or warm fluids. This procedure, called Politzerization, involved inflating the middle ear by blowing air up the nose during the act of swallowing (figure). It was not without its risks. In 1838, a quack named Turnbull caused two patients to die when using the catheter and air press. One asphyxiated from emphysema of the throat and the other died instantly, no doubt a case of air embolism.4 Though not mentioned in his atlas, MacNaughton Jones later invented cigarettes that were smoked through the nose, the aim being to pass the vapor behind the nasopharynx, or by Valsalva’s method, into the tympanum. These cigarettes, “made with a little crowsfoot leaf,” contained iodoform and eucalyptus: “the iodoform was in great measure disguised by the eucalyptus, and more so, by vanillin or coumarin.”5
MacNaughton Jones left Ireland for a very successful career at Harley Street, London, in 1883 after failing, despite his significant academic output and evident leadership skills, to gain the Chair of Materia Medica (1875) or of Surgery (1880) at Queens College, Cork. He died on 26 April 1918, aged seventy-four, at his residence at The Rest, Ravenscroft Park, High Barnet, London.
References
- McCarthy K. Stories from 1918: Medical Adventures at the Eye, Ear and Throat Hospital. http://kieranmccarthy.ie/?p=14319
- MacNaughten Jones H. Atlas of the Diseases of the Membrana Tympani: 1878. Philadelphia, Lindsay & Blakison
- https://wellcomecollection.org/works/rd2awwjt/items?langCode=eng&sierraId=b21468825&canvas=67
- Simpson JF. Joseph Toynbee: his contributions to otology. President’s Address. 1963:Proc Roy Soc Med.56:97-105
- https://blogs.ucl.ac.uk/library-rnid/2016/02/12/we-can-easily-mop-the-orifice-macnaughton-jones-and-tinnitus/
TONY RYAN, MB, MD, FRCPI, MAHTL, is a Consultant Neonatologist following 25 years at Cork University Maternity Hospital, and an Associate Professor in the Department of Paediatrics & Child Health at University College Cork, Ireland.