
Glenn Arendts
Murdoch, Australia
Coming to rest inadvertently on the ground:1 the World Health Organization (WHO) definition of a fall sounds vaguely patronizing, bordering on disinterested. The human act of staying upright is a complex triumph of the integration of neurosensory, musculoskeletal, and cardiovascular systems, and its failure is associated with injury, fear, and embarrassment. Ancient medical texts described the physical injury of long bone fractures from a fall2 and the psychological impact of the fear of falling.3 One could imagine a fall as a perfect symbol for an artist wishing to depict the fragility of humankind with age.
However when a fall is referenced in art, the fallen are mostly depicted as separated from God, with a fall the symbolic consequence of disobedience and the promotion of oneself over fidelity. In medieval and early Renaissance art, those who suffered a fall were physically capable but morally weak. Though the form may have changed over time, the fallen angel or other devotee of God still remains the most common emblem of a fall depicted in art. And as they are angels, those who have fallen are usually young.
The clinical reality of falls is very different. Those who fall are typically frail, disabled, and have multiple medical conditions. Falls are a major global health problem and are the leading cause of injurious death in people over sixty-five years of age. One third of community-dwelling older people fall annually, and a fall carries a substantial risk of further functional decline in those who are already vulnerable.4 Perhaps the only similarity these patients share with the fallen seen in art is the trait of disobedience. A little less than half of older people adhere to recommended fall prevention interventions, even in the controlled setting of a clinical trial.5
Of course, the shorter life expectancy during the fourteenth to sixteenth centuries would have limited artists’ exposure to aging and its consequences. Nevertheless, Renaissance literature is full of interesting stories of the universal human challenge of growing old, both positive and negative.6 It is a little curious that painters of that era and beyond chose to ignore one of the prime consequences of aging.
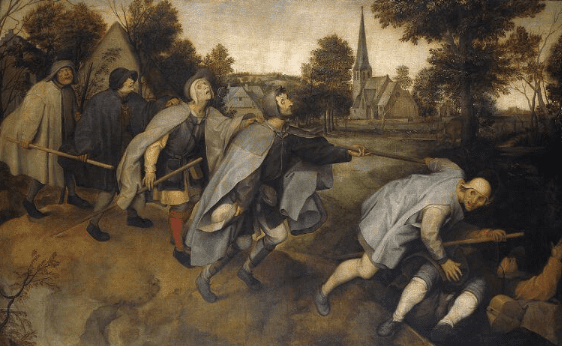
The later sixteenth century brought a change from one artist. In Pieter Bruegel’s masterpiece The Blind Leading the Blind (1568, Museo di Capodimonte, Naples), a man has fallen in a ditch. We cannot see his face, and behind him are poised grotesque representations of visual loss, each ready to follow the others into the ditch. In this painting, the fallen did not plummet from heaven, and though damned, their fall from grace has an earthly reality. The topic and composition of the painting, with the village church nestled in the background between the men already tumbling and those about to fall, has led some critics to interpret it as an attack on Catholicism and its lack of charity. I just see the tragedy and the dignity of at-risk people trying to not fall over. The faces from the back of the line to the front evolve from trust to confusion to fear; their limbs are positioned with imperfect walking sticks as the men try to stay balanced and upright; and all of this accentuated by the diagonal way their procession crosses the canvas, downhill.
Earlier, Bruegel had painted a version of The Fall of the Rebel Angels (1562, Royal Museums of Fine Arts of Belgium, Brussels), in which Archangel Michael drives Lucifer and the rebels from heaven. The “fall” in this circumstance is of course due to an external force, and so not within the WHO definition. But it was a nasty fall for Lucifer nonetheless.
That Bruegel is considered by some art historians to be the prime transforming force in the subject matter of art, allowing the stories and foibles of peasants and other common people to be revealed, is shown in these two paintings, which he painted within six years of each other. One painting is all power and fire as the damned fall to the infinity of hell; the other a sad struggle of the mortal damned on the shallow roadside.
Visual impairment remains a prominent risk for falling today, but mostly because of inappropriate use of multifocal spectacles by our patients. It is rare indeed to see the ophthalmological disasters Bruegel depicted such as bilateral eye enucleation and ocular mucous membrane pemphigoid, amongst others. Changing prevalence of disease aside, The Blind Leading the Blind has not lost its power and meaning as one of the few accurate artistic portrayals of the complexity of falls.
In the centuries that followed, painters became more accomplished at reproducing the human form, but the pain and indignity of falls in the vulnerable old remained largely untouched subjects. Falls continued to be symbolically linked to a loss of faith, even as other subjects became bolder and more pragmatic. Victorian nineteenth century painters popularized a new version of the fallen: the scandalous premarital loss of virginity by a young woman. But in terms of the reality of falls, not much changed.
Falls are really just a harbinger of a pressing health challenge faced in developed economies: how do we afford to care for the rapidly escalating number of frail elders? I am part of a team that developed an acute falls program in the largest emergency department in Australia. Older people that fall receive high level input at the front door of the hospital to identify contributing risk factors, with the goal of restoring function and independence as quickly as possible. In two years, we have managed over 4000 individuals and are now successfully discharging 20% more patients home. Inherent in our strategy is embracing the dignity of risk. Whilst we look for and manage reversible factors, we cannot eliminate falls in our older citizens, and the more zealous we become, the more we chance infantilizing the aged.
Some patients state that their first thought after a fall is akin to cringe comedy: “You’ve done it again, you stupid old so-and-so.” I tell them solemnly that falls are serious, and we should try and prevent them without restricting their enjoyment of living too much. But the truth is, some falls actually are funny. Minor twentieth century painters have sometimes depicted a fall as a social leveller, with a wealthy or superior victim brought to earth literally and figuratively. Perhaps if clinicians embraced the darkly funny, human side of falls more, we would not lose sight of what really matters to our patients when we try and “fix” our falls problem.
With this in mind, in 2019, could we have finally reached a point where some type of uneasy relationship between art and falls has been reached? Have we arrived at a postmodern truth? Last year, a man in his sixties was hospitalized after he fell into a 2.5 metre deep black hole in the floor of a museum that had been painted to look flat by the artist Anish Kapoor (Descent Into Limbo, 1992, Serralves Museum, Porto). I wonder, could art leading to a fall be the backlash to centuries of falls failing to lead to art?
References
- https://www.who.int/violence_injury_prevention/other_injury/falls/en/
- Disease in Ancient Egypt and Nubia, by Joyce Filer. British Museum Press (1995)
- Fear of Flute Girls, Fear of Falling by Helen King. In Mental Disorders in the Classical World https://doi.org/10.1163/9789004249875_014 (2013)
- Nagaraj G, Hullick C, Arendts G, Burkett E, Hill KD, Carpenter CR. Avoiding anchoring bias by moving beyond ‘mechanical falls in geriatric emergency medicine. Emergency Medicine Australasia 2018; 30(6): 843-850
- Nyman SR, Victor CR. Older people’s participation in and engagement with falls prevention interventions in community settings: an augment to the Cochrane systematic review. Age and Ageing 2012; 41(1); 16–23
- Aging Gracefully in the Renaissance: Stories of Later Life from Petrarch to Montaigne by Cynthia Skenazi. https://doi.org/10.1163/9789004255722 (2013)
GLENN ARENDTS, MBBS, MMed, PhD, FACEM, is an emergency physician with a clinical research program designed to improve patient centred outcomes for older people in ED. He has published over 100 peer review articles and was the foundation chair of the Geriatric Emergency Medicine Interest Group of the Australasian College for Emergency Medicine.