
Mark Gilbert
Halifax, Nova Scotia, Canada
James E. Van Arsdall
Omaha, Nebraska, United States

I first met Scottish artist Mark Gilbert in 2013 as a participant in his Ph.D. dissertation study, “The Experience of Portraiture in Clinical Settings” [EPICS]. I was introduced to the study during a follow-up appointment with my head and neck cancer surgeon. Twelve years earlier, at the age of fifty-three, I was diagnosed with squamous cell carcinoma on my tongue, which was removed surgically along with corresponding lymph nodes. I also underwent radiotherapy. Prior to EPICS, Mark had collaborated with physicians and patients on several projects that sought to use art, specifically portraiture, to explore notions of illness, recovery, care, and caregiving.1,2 During these studies, Mark became acutely aware of how fundamental the intimate nature of the relationships and interactions between participants and himself were to the portrait-making process. He realized the connections made with each person were as diverse as the participants themselves and responded to their voices, both silent and spoken, to guide and inform the marks he made on the canvas.2
This realization inspired EPICS, which explored the patient experience of participation in the portraiture process in a Head and Neck Cancer Clinic.3 I had initial doubts about the project; I had not been drawn before and never envisaged that sitting for my portrait would be part of my experience at the Head and Neck Cancer Clinic. But I was curious to meet Mark and interested in what the study might reveal.
All the portrait sessions took place in the same clinic I had attended for the past fifteen years to receive care for osteoradionecrosis (non-healing bone after radiation), dry mouth, enlarged lymph nodes, swallowing problems, and the other effects of my treatment. In total, I visited his studio seventeen times over a three-month period.
At the end of the first scheduled portrait session (fig 1), I was given a journal and asked to record any thoughts or stories relating to, or triggered by, my participation or the portraits themselves. In the journal, I also considered potential healing qualities of our portrait process.
I was puzzled and perplexed by the project at first; I did not totally understand what it was about. At times, I was confused about where the whole process was going, which actually paralleled my experiences with my cancer and treatment. However, Mark and I worked through these uncertainties together, in much the same way as my surgeon and I tackled the challenges of my treatment.
Mark and I got to know one another during the many sessions together. Developing personal relationships has been a part of my entire treatment for cancer and side-effects. I have had fantastic relationships with all the health professionals involved in my treatment over the years and the portraiture process has deepened those bonds. A trusting, collaborative, and reciprocal relationship between the artist and the sitter is required.3 Moreover, although I never met any of the other participants, I felt I got to know them as I sat for Mark. Looking at their portraits as they developed made me feel associated with them and I realized that I was not alone.
All participants reported that the studio became a comfortable place to contemplate, to be heard, and to express themselves. For me the studio became not only a physical space but also an emotional and spiritual space. The sessions with Mark gave me an opportunity for self-examination and contemplation of the years since my original diagnosis, something I had not done before. Usually I came to the clinics for more treatment or follow-up, but those visits never involved self-reflection. The portraiture process made me think more about me. The opportunity for self-reflection through looking at so many pictures of myself was a valuable part of the project for me.
Participation involved being more intensely reflective than ever before. As Mark and I talked, I was in a constant process of reflection, but I was also trying to consciously build a narrative and find purpose and meaning in my reflections. I described my portrait as a manifestation of my self-analyses and contemplation and recognized a mystery within the project and within myself. There are many cancer support groups, some of which I participated in during the early days of my diagnosis and treatments. None of these allowed me the opportunity to share and reflect in the way EPICS did.
I relished the other participants’ portraits; seeing them gave me a sense of comradeship with others who have gone through a very similar struggle. I know they all have a story too, and I would like to know what it is. I look at all these faces, including my own, and wonder how they did.
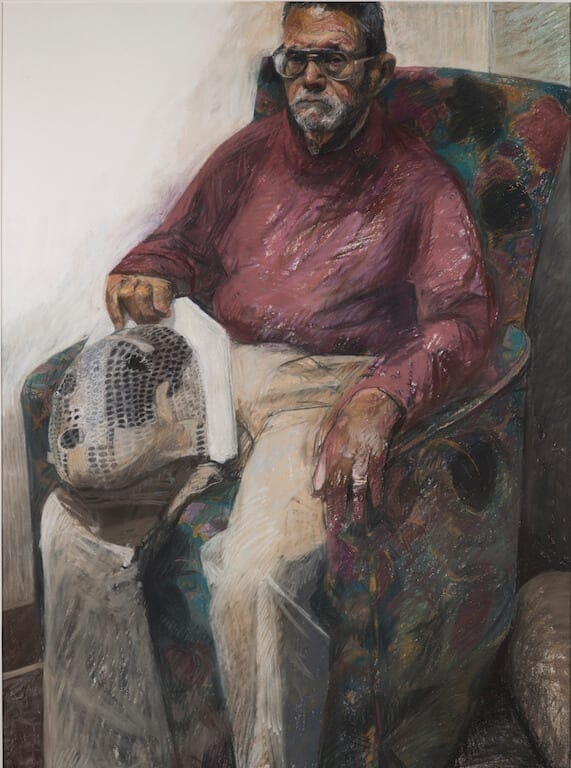
As a member of the Institute for Cultural Connections at a local college, I see the potential for these portraits to be a testament to my life. I regard my larger, more elaborate pastel portrait with my mask as more historical (Fig 2). It harbors memories of my treatments, the steps I went through, and the portraiture process. My radiotherapy mask profoundly symbolized the journey I had taken over the years since my diagnosis. During the project I realized my potential to influence the choices Mark made as he constructed the portraits. I often discussed with Mark how the mask was symbolic of my treatment and recovery. I recognized that what I said, did, and felt could manipulate the resultant shape of the portrait. I even commented on the fact that I could sway the nature and structure of the portraits, recognizing, “I am obviously trying to influence you . . . to influence your interpretation.”
Sitting for my portraits opened a space to figuratively stand at my own easel, to tell my story and step back to allow for whatever might surface. Participation enabled me to share stories with the artist, those I work with, and other members of my community. I was able to use photographs I took of the portraits as they progressed to talk about my medical journey. This helped others to know a little more about me. I shared my portraiture experience with my wife and my colleagues at work.
They asked me questions about myself that they would not have thought to ask before, and it forced me to answer them. Many people did not realize how long I had been receiving treatment until I shared the photographs of the art work.
A public exhibition of the portraits would be an opportunity to more extensively share all our stories. I have advocated for an exhibit at my local community college because I want to be involved in displaying the project. The other participants also wished to share their stories and to spread the message that they were not only survivors, but also thriving, lively, active individuals.
Our involvement in this study provided us with the opportunity to explicitly engage in our own healing journey. As a result of this process, I have found time to revisit and come to terms with aspects of my illness and healing experiences. The studio space gave me the opportunity to relax, reflect, take stock, and attend to aspects of my life that were unpredictable, challenging, comforting, and upsetting. I have woven them into my own story and portrait, which was therapeutic and empowering.
The future
I was one of five subjects involved in this project. I have yet to meet the other participants but I hope to meet them as we plan the public exhibition. The portrait exhibition will serve as testimony to the stories we all shared in Mark’s tiny studio in the clinic, and create a new space for others to engage with our stories and reflect on their own. These reflections may enable the viewer to engage with what we ourselves have found challenging and isolating, and transform those experiences into something that is communal, healing, and empowering.
Note
In 2014 just after having surgery to rebuild his jaw he met Scottish artist Mark Gilbert. In total, he visited Dr. Gilbert’s studio 17 times over a 3-month period.
References
- Aita VA, Lydiatt WM, Gilbert MA Portraits of care: medical research through portraiture. Medical Humanities 2010;36:5-13.
- Gilbert M. Experience of portraiture in a clinical setting: An artist’s story. Journal of Applied Arts & Health 2014;5:1:135-150.
- Gilbert MA, Lydiatt WM, Aita VA, et al Portrait of a process: arts-based research in a head and neck cancer clinic Medical Humanities 2016;42:57-62.
MARK GILBERT, PhD, is a researcher and artist and has worked on a number of arts based collaborations with patients and caregivers. In 2014 he received his PhD from University of Nebraska Medical Center. He continues to explore the relationship between art and medicine, and is currently the recipient of a Post Doctoral Fellowship in the division of Medical Education at Dalhousie University, Nova Scotia, Canada.
JAMES VAN ARSDALL, EdD, is a faculty member at Metropolitan Community College in Omaha, Nebraska where he teaches political science, military history, Latin American history, and world civilization courses. Dr. Van Arsdall received his BS degree in History and Political Science from Western Carolina University and his MA and Ed.D. degree from the University of Nebraska in Comparative/International Education and Adult Education Policy Studies.