
In some respects the year 1860 represents a watershed in the history of surgery. It was the year when a young surgeon from the Edinburgh Royal Infirmary by the name of Joseph Lister came to the University of Glasgow to take up the position of Regius Professor of Surgery. It was also a time when surgery was emerging from its semi-barbarous medieval state owing to the introduction and widespread acceptance of general anesthesia. Yet on the wards of the average hospital the odds of a patient surviving a surgical operation were about the same as escaping alive from fighting Napoleon on the battlefield of Waterloo almost fifty years earlier.
Indeed on these surgical wards wound infections spread from patient to patient like wildfire. No surgeon could ever be certain that his patient would survive his surgery. Compound fractures were the surgeon’s nightmare, often ending up in “hospital gangrene” and amputation. The death rate from major surgical operations or limb amputation was as high as 40%, rising to 60% in French hospitals. Even simpler operations carried a high risk of death from infection. The hospitals were blamed for this, and there was much talk of closing them down and having the patients being taken care of at home. In Nuremberg, the city fathers seriously considered pulling down the Allgemeines Krankenhaus.
Hygiene in hospitals was deplorable. A haunting mildly nauseating smell of putrefaction clung to the clothes of the surgeons, some of whom were not ashamed to speak of the “good old hospital stink.” Old rags were strewn about the operating room, also sponges and dirty instruments. Surgeons rarely washed their hands; wore street clothes while operating; and circulated freely between the living patients they treated and the dead ones they dissected or autopsied. No attempt was made to isolate septic cases, and the nurses and dressers moved directly from patients with erysipelas to healthy ones. The water supply was often polluted, and toilets could be placed in close proximity to the patient area. A hospital was not expected to be more spotless than a carpenter’s shop.
According to the prevailing theory of the time, wound infections (“putrefaction”) were attributed to gases (chiefly oxygen) entering the wound and causing tissue breakdown. Opinions varied as to how the air became tainted, but the observations of Semmelweiss had made no impact on the conservative medical establishment of the time. No surgeon ever risked opening an abdomen or entering a joint. Abscesses were left unopened, rarely drained, or treated by making incisions with valvular openings that would prevent the entrance of oxygen.
But in France a rising young chemist, Louis Pasteur, was about to unleash a great revolution. He had studied milk, wine, beer, silkworms, and yeasts. Between 1850 and 1860 he had performed a series of rigorous experiments that led him to conclude that the souring of milk by the production of lactic acid and the conversion of glucose to ethanol to make wine were initiated by living microscopic organic matter present in the air. None of these processes would take place when air was excluded from the media in which these experiments were conducted. Pasteur then demonstrated that putrefaction of organic matter such as dead meat would also not in occur when air was excluded, indicating that this too was caused by the matter present in the air; and it was his genius to make the final leap that human diseases occurring during life would also be caused by aerially transmitted germs.
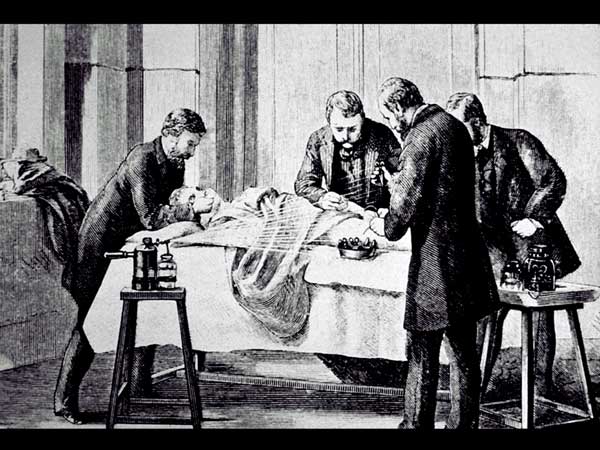
Surgery using Lister’s carbolic acid sprayer
So it was at a propitious time that young Joseph Lister came to Glasgow. Born in London in 1827 into a Quaker family, he had been exposed to science since boyhood. Trained by his father to use microscopes, he had studied microscopic fungi and other botanical specimens, dissected small animals, and articulated skeletons. He went to two private schools, and had learned French and German, chemistry, physiology, botany, and microscopy. He had trained under distinguished professors of medicine and physiology, graduating from the University of London in 1852 and later becoming a fellow of the Royal College of Surgeons. While at University College he had written papers on the muscle of the iris and the involuntary muscle fibers of the skin; and had witnessed there the first surgical operation done under ether anesthesia. After graduation he moved to Edinburgh (1853), secured a surgical appointment at the University and the Royal Infirmary, married his chief’s daughter, and spent the next seven years operating, lecturing, and engaging in research. In 1860 he was appointed Regius Professor at the University of Glasgow.
For years Lister had impressed on his students the marked difference in outcome between simple fractures, when the skin was intact, and compound fractures, in which the surface of the skin was broken and amputation was common. One afternoon in 1864, while walking home with a colleague, the professor of chemistry, the latter drew his attention to one of Pasteur’s papers. From that he learned that fermentation and putrefaction were caused not by the gases of the air but by living particles floating in it and settling down on surrounding objects. If these primitive forms of life could be destroyed by boiling, then why not by chemicals? Indeed, “antiseptic” substances had been used since time immemorial, even by the early Egyptians, and probably also before that. Alcohol had been used freely on the continent, also at times “oil and wine,” glycerin, chlorine, iodine, and coal tar. By 1851 carbolic acid had been used in England to preserve cadavers, and in 1860 Jules Lemaire in Paris had published on its use in the treatment of wounds but was largely ignored. All these agents, moreover, were used for treatment, not prevention.
After reading Pasteur’s paper Lister conceived the idea of preventing surgical infections by destroying the organisms that caused it. He settled on a substance called German creosote, used to clean up a sewage plant in nearby Carlisle and then available as a 5% carbolic acid solution. For his first patient, one with a compound fracture of the leg, he produced a small bottle of carbolic acid, poured some into the wound and made a paste of it by mixing it with the blood, then covered the wound and added some fresh carbolic acid every day. The patient recovered with no infection. Between 1865 and 1867 he treated eleven cases of compound fractures, of which nine healed without infection. Next he successfully removed a tumor from a man’s arm by applying his antiseptic to the sutured wound; then used it for several amputations, also for a large ventral hernia that required removing a great amount of fat. As carbolic acid was irritating in solution, Lister dissolved it in oil and later mixed it with powdered chalk to form a sort of a paste or putty that was applied to the wound. To prevent secondary hemorrhage he also used carbolic acid to sterilize the gut suturing material.
After 1870, not being wedded to carbolic acid, Lister used absorbent gauze impregnated with various other antiseptic substances. Between 1871 and 1887 he also used a carbolic acid spray to purify the air in the operating room. It was a pump with a long handle that came to be called the “donkey engine” and caused much mirth but was abandoned when Lister realized that pathogenic organisms were not plentiful in the air. In fact, at a meeting in Berlin in 1890, he said that “As regards the spray, I am ashamed that I should ever have recommended it for the purpose of destroying microbes in the air.”
At first Lister’s antiseptic approach met a mixed reception. Acclaimed by his staff and by those who had studied the details of his technique, it was highly praised in Germany and most other countries, but not in London. In 1869 he left Glasgow to become professor of surgery in Edinburgh. Then in 1877 he accepted an invitation to become professor of surgery at King’s College Hospital in London, largely because he felt it was his mission to promote his method. But the London surgeons were neither impressed nor persuaded. One surgeon while operating sarcastically asked the nurses to close the door, so as not to allow Mr. Lister’s germs to come into the room. The nurses also grumbled and were difficult to work with, being accustomed to regard the wards as their private domain into which no man should come without their permission and interfere with any of their arrangements, such as ventilation or the ways they dressed the wounds. But Lister prevailed. His reputation grew. The surgeons were converted. By 1890 the whole world had accepted Lister’s great innovation, and by then the microbes causing sepsis had been identified and cultured.
Eventually most surgeons abandoned antisepsis and switched to the aseptic technique, which Lister pointed out was just a modification of his antiseptic methods and sometimes indeed needed antiseptic support. He made other improvements to surgery, useful surgical instruments, an aortic tourniquet, and was the first to use carbolic acid to treat varicose veins. He was also the first surgeon in Britain to use a rubber drainage tube, the patient in question being Queen Victoria. Many honors were showered on him; he retired from active surgery in 1893, was elected President of the Royal College of Surgeons in 1895, and made a baronet in 1897. He died in 1912. He is remembered as the innovator who revolutionized the history of surgery, dividing it into the era that came before him and the era that came after him.
References
- British Medical Journal. May 29, 1897; Dec 13, 1902; Sept 27, 1924; May 16, 1925; Apr 9, 1927; Apr 1, 1967.
- Clark PF, Joseph Lister, his life and work. The Scientific Monthly 1920; 11:518.
- Ford WW, The bacteriological work of Joseph Lister. The Scientific Monthly 1928; 26:70.
- Harley, Williams, Masters of Medicine, PAN-Books Ltd,1954.