
Marilyn Napolitano
Scottsdale, Arizona, United States
A storied connection exists between religion and medicine. The first hospitals were monasteries and convents, where holistic care tended to spiritual needs alongside those of the body. From the Middle Ages on, religious orders played a major role in the founding of medical institutions. Between 1866 and 1926 alone, nuns established almost 500 healthcare institutions in the United States.1 Today, many institutions still bear the name of a saint or other title reflecting religious affiliation.
Medical buildings managed by religious orders often demonstrated the creation of a “sacred space.” The Hôtel-Dieu in Beaune, France, founded in 1443 and run by the Catholic Church for centuries, is a primary example. Called a “palace for the poor,” the main ward included brightly painted ceiling beams, ornate tiled floors, and luxurious beds with vibrant red sheets. At the end of a long hall was an intricately carved stone altar, placed so that patients could attend Mass in bed, and crowned with a polyptych altarpiece painted by Rogier van der Weyden depicting the Last Judgement.2 Hôtel-Dieu served as a place of peaceful repose, providing also what would be termed hospice care today. It was designed for patients to reflect on both mortality and eternity through visual art and architecture while receiving physical care and nourishment.
Visual art within healthcare spaces offers an even more intimate connection between the divine and healing. For example, an icon is a religious image used for veneration and prayer depicting a holy person, such as a saint, painted in a stylized manner that originated in the Byzantine Empire.3 Those who suffered for their faith are often shown with the cause or instrument of their death through recognized symbols; St. Stephen, for instance, is commonly painted with a basket of stones.4 Saints may also be recognized as “patrons” for specific groups or medical pathologies: St. Blaise for throat disease; St. Agatha for patients with breast tumors5,6; St. Jude, the eponymous saint of the famous Children’s Research Hospital, is invoked for “lost causes.”7
How does the depiction of saints through iconography promote healing? One way is by providing a visual language for suffering. Pain is represented through the image of a suffering martyr, a visual reality for invisible feelings and sensations. Visual art is employed in psychological interventions such as art therapy8 and storytelling.9 Using art to tell a story can be helpful when patients struggle to express their suffering verbally. Physical pain, as Elaine Scarry writes in The Body in Pain, “does not simply resist language but actively destroys it.”10 Thus, when patients are limited by the “pre-verbal” nature of pain, the icon gives a bridge to expression as well as validation of internal suffering. Patron saints also provide a sense of connection and comfort through community by representing a group of people undergoing difficult trials.
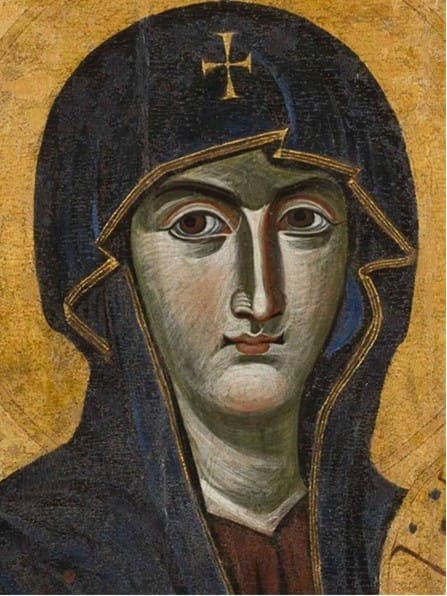
Presence is also created by the artistic style of iconography itself. The figure stares directly ahead, eyes watchful and unblinking. Traditionally, the pupils were the darkest point on the face, painted completely black with no reflection, to draw one’s gaze.11 As Kristen Drahos notes, “Unlike pictures, the icon offers a ‘full-face address.’”12 While evoking a person, icons are not meant to be realistic portrayals of those they depict. The faces are heavily stylized, with disproportionately large eyes, long thin noses, and tiny mouths. Icons are dynamic images that viewers engage with, the goal being not only to look at an icon, but through it.
The use of sacred imagery to provide hope is not merely a relic of history; rather, it aligns with modern clinical findings regarding the power of images to impact patient outcomes. Visual art can positively affect clinical measures such as stress levels and blood pressure and is the basis behind the field of “evidence-based design.”13 Art in hospitals is an environmental element that influences patient experience. Studies show that humans generally prefer landscapes and depictions of nature, which also have a more positive impact on emotional and physiological stress.14
Art in hospitals can also provoke thought and dialogue. Art At the Bedside, a program initiated by Susan Daiss, chaplain at the University of Rochester, uses images as “conversational mediators.” Patients select and view a library of images related to a chosen theme, followed by a guided discussion. Findings from the program showed wide-ranging benefits from warding off boredom to allowing patients to communicate about their illness and reflect with family members.15
Starting a dialogue is especially important when it comes to harder topics such as death and dying. End-of-life conversations are associated with less aggressive care near death, earlier hospice referrals,16 and higher rates of advanced care planning, which ensures that the patient’s wishes are honored and reduces stress for families.17 This relates to a concept commonly represented in sacred art—that of memento mori. Latin for “remember your death,” it is the idea that death is universal and unavoidable, encouraging viewers to engage with their own mortality, and, for believers, to reflect on the eternal nature of their soul.18 The Last Judgement altarpiece in the Hôtel-Dieu exemplifies this concept, as does the historical use of more overt symbols like skulls and skeletons in art.

Art can also ease discomfort for healthcare workers when initiating end-of-life discussions. In the Memento Mori workshop, sixteen art pieces were viewed and discussed in small groups of nursing students. Most found that the art encouraged deeper exploration of their personal beliefs about death, as well as promoted empathy for the perspectives and experiences of others.19
These findings suggest there is still a place for sacred art in modern medicine. Research on the role of spirituality in health suggests that religious beliefs influence a patient’s understanding of their illness and impact medical decision-making.20 Patients often want physicians to ask about their spiritual beliefs, although they rarely do.21,22 But whether or not a patient expresses their religious or spiritual beliefs, sacred art may serve a purpose. Icons, for example, have the potential to foster “interreligious exchanges and secular moments of encounter.”12 Sacred art can move beyond its theological meaning to express broader psychological and social themes.
Whether sacred or secular, art has a powerful function in the clinical space, providing comfort and hope but also promoting dialogue. The themes of suffering and death prevalent in sacred art address universal human experiences that transcend culture or creed. By using art to navigate these difficult topics, medical professionals can enhance communication and connection for patients, their families, and healthcare workers. Art is an element of a more holistic model of care, one that acknowledges each patient as an individual, not just a body to be cured. Much like the reflective environment of the Hôtel-Dieu or the unblinking eyes of a Byzantine icon, modern healthcare spaces can utilize architecture and visual imagery to ensure patients feel recognized in the fullness of their humanity.
References
- Wall, Barbara Mann. “Hospitals and Habits: Catholic Sisters and the Medical Marketplace, 1860-1930.” American Catholic Studies 116, no. 1 (2005): 91–94. http://www.jstor.org/stable/44194869.
- Shipman, Kate Elizabeth, and Sudarshan Ramachandran. “The Hôtel-Dieu de Beaune, a Testament to the Health Benefits of Religious Charity and Vineyards.” Hektoen International, 2015. https://hekint.org/2017/02/23/the-hotel-dieu-de-beaune-a-testament-to-the-health-benefits-of-religious-charity-and-vineyards/.
- Cartwright, Mark. “Byzantine Icons.” World History Encyclopedia, December 8, 2017. https://www.worldhistory.org/article/1161/byzantine-icons/.
- Lanzi, Fernando, and Gioia Lanzi. Saints and Their Symbols: Recognizing Saints in Art and in Popular Images. Collegeville, Minn: Liturgical Press, 2004.
- Britannica Editors. “St. Blaise.” Encyclopedia Britannica, January 30, 2026. https://www.britannica.com/biography/Saint-Blaise.
- Britannica Editors. “St. Agatha.” Encyclopedia Britannica, February 4, 2026. https://www.britannica.com/biography/Saint-Agatha.
- Britannica Editors. “St. Jude.” Encyclopedia Britannica, October 9, 2025. https://www.britannica.com/biography/Saint-Jude-Apostle.
- Barnett, Kelly Sarah, and Fabian Vasiu. “How the Arts Heal: A Review of the Neural Mechanisms behind the Therapeutic Effects of Creative Arts on Mental and Physical Health.” Frontiers in Behavioral Neuroscience, October 2, 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11480958/#s5.
- Rita, Charon. “Narrative and Medicine.” The New England Journal of Medicine, 2004. https://pubmed.ncbi.nlm.nih.gov/14985483/.
- Scarry, Elaine. The Body in Pain: The Making and Unmaking of the World. New York: Oxford University Press, 2006.
- Mitrović, Todor. “The Epiphany of the Eye.” Orthodox Arts Journal, June 15, 2021. https://orthodoxartsjournal.org/the-epiphany-of-the-eye/.
- Drahos, Kristen. “Beyond Medical Pathography: Iconographic Pathography as Transfigured Storytelling.” Horizons 51, no. 2 (November 25, 2024): 303–25. https://doi.org/10.1017/hor.2024.26.
- Nielsen, Stine L., Lars B. Fich, Kirsten K. Roessler, and Michael F. Mullins. 2017. “How Do Patients Actually Experience and Use Art in Hospitals? The Significance of Interaction: A User-Oriented Experimental Case Study.” International Journal of Qualitative Studies on Health and Well-Being 12 (1). https://doi.org/10.1080/17482631.2016.1267343
- Ulrich, Roger S. 1986. “Human Responses to Vegetation and Landscapes.” Landscape and Urban Planning 13 (January): 29–44. https://doi.org/10.1016/0169-2046(86)90005-8.
- Daiss, Susan Dodge-Peters. 2016. “Art at the Bedside: Reflections on Use of Visual Imagery in Hospital Chaplaincy.” Journal of Pastoral Care & Counseling Advancing Theory and Professional Practice through Scholarly and Reflective Publications 70 (1): 70–79. https://doi.org/10.1177/1542305015618170.
- Wright, Alexi A. 2008. “Associations between End-of-Life Discussions, Patient Mental Health, Medical Care near Death, and Caregiver Bereavement Adjustment.” JAMA 300 (14): 1665. https://doi.org/10.1001/jama.300.14.1665.
- Wilson, Eleanor, Glenys Caswell, Nicola Turner, and Kristian Pollock. 2022. “Talking about Death and Dying: Findings from Deliberative Discussion Groups with Members of the Public.” Mortality 29 (1): 1–17. https://doi.org/10.1080/13576275.2022.2136515.
- Shaw, Joseph. 2023. “Memento Mori: Death in Christian Tradition.” Catholic Answers. 2023. https://www.catholic.com/magazine/online-edition/memento-mori-why-you-should-remember-to-die.
- Nicol, Jane, and Mary Pocock. 2020. “Memento Mori: Can Art Assist Student Nurses to Explore Death and Dying? A Qualitative Study.” Nurse Education Today, March, 104404. https://doi.org/10.1016/j.nedt.2020.104404.
- Puchalski, Christina M. 2014. “The FICA Spiritual History Tool #274.” Journal of Palliative Medicine 17 (1): 105–6. https://doi.org/10.1089/jpm.2013.9458.
- Ehman, John W., Barbara B. Ott, Thomas H. Short, Ralph C. Ciampa, and John Hansen-Flaschen. 1999. “Do Patients Want Physicians to Inquire about Their Spiritual or Religious Beliefs If They Become Gravely Ill?” Archives of Internal Medicine 159 (15): 1803. https://doi.org/10.1001/archinte.159.15.1803.
- McCord, G. 2004. “Discussing Spirituality with Patients: A Rational and Ethical Approach.” The Annals of Family Medicine 2 (4): 356–61. https://doi.org/10.1370/afm.71.
MARILYN NAPOLITANO is a third-year medical student at the Mayo Clinic Alix School of Medicine in Scottsdale, Arizona.