
Piyush Pillarisetti
Pennsylvania, United States
Achalasia is an esophageal motility disorder characterized by impaired lower esophageal sphincter (LES) relaxation and absent or spastic esophageal peristalsis. Typically, the condition leads to solid and liquid dysphagia at symptom onset. After the pathophysiology of achalasia was described in the 1900s, treatment modalities have converged on one goal: reduce LES tone, thereby hastening transit of food across the sphincter to the stomach. In current practice, there are several treatment modalities that serve this purpose with varying degrees of efficacy, such as nitrates, calcium channel blockers, botulinum injections, Heller myotomy, pneumatic dilation, and per-oral-endoscopic myotomy. These modern treatments represent the work of nearly 350 years of incremental advancements in how to effectively treat the symptoms of achalasia.
Before the characterization of the pathophysiology by Hurst and Rake in 1929, achalasia was a clinical diagnosis based on the hallmark symptoms of progressive dysphagia, food regurgitation, and food impaction. The condition was thought to result from intermittent spasm of the cardiac region of the distal esophagus and was therefore coined “cardiospasm.” Consequently, until the early 1900s, treatment modalities for achalasia were the same as those used for esophageal strictures.
The first documentation of “cardiospasm” in the medical literature and its treatment is attributed to Thomas Willis, an English physician and founding member of the Royal Society, in 1674.1 At the time, the dysphagia observed in cardiospasm would have been viewed as a manifestation of esophageal obstruction. Willis’s treatment approach entailed 1) attaching a sponge to the end of a whalebone shaft (at the time, mostly used for making canes and corsets), 2) passing the whalebone through the esophagus, and 3) using the sponge at the distal end of the whalebone to relieve areas of resistance. Because esophageal narrowing is not a feature of achalasia, it is unlikely that the sponge would have encountered resistance in the esophagus or provided symptom relief for patients. One can also imagine the complications of such an approach. With such a long lever in a pre-sterilization era, slight changes to the angle of the whalebone during the procedure could disproportionately affect the magnitude of radial displacement at any point, posing a significant risk of esophageal perforation and infection.
France, in the early 1800s, bore witness to cardiospasm’s next treatment modality: the mechanical bougienage. Unlike the non-uniform whalebone shaft used by Willis, the mechanical bougienage approach required the physician to pass a circumferentially uniform, rigid bougie through the esophagus to condense any strictures along its descent.2 Again, as strictures are not a feature of achalasia, this approach also likely had limited efficacy for patients with cardiospasm.
In 1887, balloon dilation was introduced as a new treatment for cardiospasm in Britain. This technique involved 1) attaching an inflatable rubber balloon covered in silk to the distal end of a bougie, 2) passing the bougie through the esophagus, and 3) inflating the balloon at the distal end to increase the esophageal lumen diameter.3 Although not explicitly documented, it is possible that dilation occurred at the cardia, thereby expanding the LES and providing some symptomatic relief. This approach bears resemblance to and laid the groundwork for the modern technique of pneumatic dilation.
The early 1900s marked one of the biggest watershed moments in the treatment of “cardiospasm,” with Ernst Heller performing the first myotomy in 1913. At this time, it was thought that cardiospasm was due to the cardia of the esophagus experiencing intermittent spasms, preventing food passage through the LES. Despite being unaware of the precise pathophysiology of the disease, Heller proposed that by cutting the muscle fibers of the LES, food would more easily pass through to the stomach. Initially wanting to perform a gastroesophageal anastomosis based on Heyrovsky’s approach, Heller eventually decided on myotomy. Via open surgery, he cut the LES muscle longitudinally along the anterior and posterior planes while sparing the mucosal layers and successfully surgically reduced LES tone.4 The Heller myotomy, for the first time, represented a long-term solution to achalasia, and would set the stage for subsequent minimally invasive myotomy approaches. Because LES tone is significantly reduced with myotomy, patients often need to take acid suppression medications for post-operative acid reflux. The Heller myotomy continues to be performed in the modern era, albeit with the addition of fundoplication to reduce reflux.
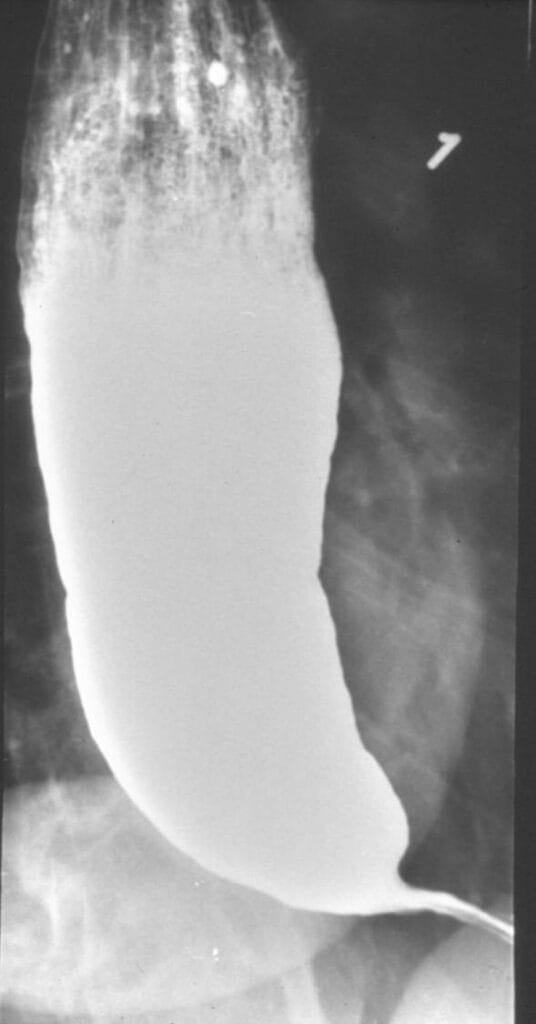
The pathophysiology of achalasia was eventually described in 1929 by Hurst and Rake.5 Using barium radiographs, they found that the distal esophagus was significantly dilated in patients with achalasia, evidenced by failure of barium passage across the LES. Normally, the swallowing reflex reduces LES tone and would allow barium to transit through the LES. This was not seen in those with achalasia. They proposed that achalasia is, in fact, not due to a mechanical obstruction but occurs because of a failure of LES relaxation. Later researchers used histopathological studies to advance understanding of this mechanism, finding that degeneration of ganglion cells in the Auerbach plexus, which are nestled in between the longitudinal and circular muscular layers of the LES and normally secrete nitric oxide to relax the LES, results in the inability of the LES to relax in achalasia.
The mid-1900s saw a major advancement in the diagnostic evaluation of achalasia with the introduction of esophageal manometry, which involves inserting a coated pressure-transducer catheter through the esophagus to measure esophageal and LES pressures during swallowing.6 This enabled a more quantitative diagnosis of the disease.
Pneumatic dilation, which utilizes air-inflated balloons to dilate the LES, rose to prominence as an effective nonsurgical treatment option between 1960–1990 and continues to be used in modern-day practice.7 In this approach, an air-filled balloon is passed down the esophagus, nestled in the LES, and inflated. A major limitation that was yet to be addressed was the risk of esophageal perforation and trauma to the sphincter. This was, in large part, due to the inability to visualize the esophagus or LES during the procedure. This limitation was addressed with the development of endoscope-guided balloon inflation in the 1990s, which allowed for direct visualization of the LES during dilation, making the treatment of achalasia markedly safer and more efficacious.8 The mid-1990s also saw the use of endoscopic botulinum toxin injections for achalasia.9 Often used as a bridge for patients awaiting pneumatic dilation or myotomy, or for patients deemed poor surgical candidates, botulinum toxin is injected into the LES to reduce sphincter tone, temporarily providing symptomatic relief.
In 2006, the use of per-oral-endoscopic myotomy (POEM) marked another pivotal development in achalasia treatment after the Heller myotomy. In contrast to laparoscopically performed Heller myotomy, POEM offered a minimally invasive, endoscopic alternative. The procedure involves first creating a submucosal tunnel in the esophageal wall, followed by myotomy of circular muscle fibers of the LES.
The historical progression of achalasia treatment from Heller’s whalebone shaft to POEM illustrates that deciphering disease pathophysiology is absolutely critical to the development of physiologically grounded and efficacious interventions.
References
- Willis, Thomas. Pharmaceutice rationalis sive diatriba de medicamentorum operationibus in humano corpore. Vol. 2. De Tournes, 1979.
- Vareliaud, A. “Observations sur un retrecissement de I’oesophage et description d’un procede nouveau du citoyen boyer pour des sondes elastiques dans ce conduit. L’introduction.” J Med Chir Pharm 1 (1801): 139-150.
- Stoker, David L. “Evaluation of oesophageal reflux.” Annexe Thesis Digitisation Project 2016 Block 6 (1990).
- Heller, E. “Extramuköse cardiaplastik beim chronischen cardiospasmus mit dilatation des oesophagus.” Mitt Grenzgeb Med Chir 27 (1914): 141-149.
- Hurst, Arthur F., and Geoffrey W. Rake. “Achalasia of the cardia: so-called cardiospasm.” QJM: Quarterly Journal of Medicine 92 (1930): 491-508.
- Fe, Fyke. “The gastroesophageal sphincter in healthy human beings.” Gastroenterologia 86 (1956): 135.
- Vantrappen, G., J. Hellemans, W. Deloof, P. Valembois, and J. Vandenbroucke. “Treatment of achalasia with pneumatic dilatations.” Gut 12, no. 4 (1971): 268-275.
- Lambroza, Arnon, and Robert W. Schuman. “Pneumatic dilation for achalasia without fluoroscopic guidance: safety and efficacy.” American Journal of Gastroenterology (Springer Nature) 90, no. 8 (1995).
- Pasricha, PankajJ, WilliamJ Ravich, and AnthonyN Kalloo. “Botulinum toxin for achalasia.” The Lancet 341, no. 8839 (1993): 244-245.
PIYUSH PILLARISETTI is a third-year medical student interested in the medical history of current medical treatment modalities, with a focus on how past innovations inform present-day clinical care.