
JMS Pearce
Hull, England
Few illnesses convey more fear of a swift, fatal outcome than does meningitis. Cerebrospinal meningitis was once known as spotted fever, cerebrospinal fever, typhus cerebralis, or meningitis epidemica. In Greek meninx, or in Latin meningeus, is a membrane. In English literature, meninges appeared in 1543: “Whan the brayne pan is remoued, there appere two rymes, or thynne skynnes, called in greke meninges.”1 John Bell, in Anatomy of Human Body (1797) used the word meningeal to describe “the arteria meningea, the great or middle artery of the dura mater.”
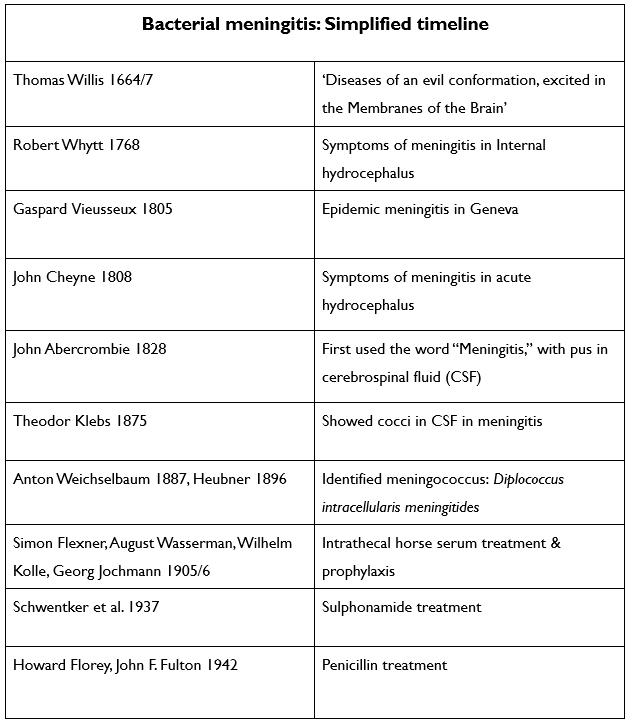
Although the Oxford English Dictionary cites the earliest use of the word meningitis as 1824, Thomas Willis (1621–1675) clearly described the “deadly distemper” if not the word:
Difeafes of an evil conformation, excited in the Membranes of the Brain, by which, at firft for a long time, frequent Headaches, and moft cruel, and then afterwards a fleepy and deadly diftemper hath been induced the caufe of the Difeafe not detected, but after death by Anatomy.2
One of his patients had obstructive hydrocephalus caused by meningitis shown at autopsy when the brain “abounded with a watery humour.” Willis recorded in Pathologiae Cerebri (1667) “Epidemical fever chiefly infectious to the Brain and nervous Shock” that occurred in Oxford in 1661; the description is consistent with meningoencephalitis of uncertain cause.
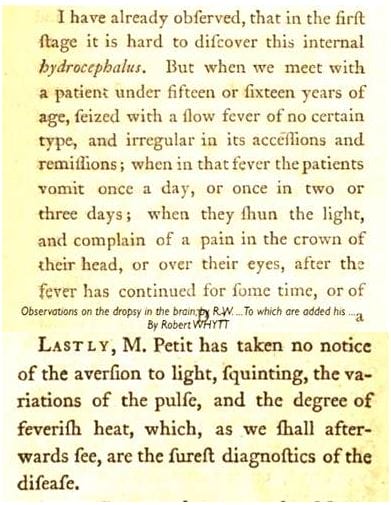
Coherent clinical accounts by Whytt, Cheyne, and Abercrombie were to follow, though some were ascribed to hydrocephalus.3 In his 1768 book, published posthumously, Robert Whytt (1714–1766) described headache, fever, and photophobia—symptoms typical of meningitis:
John Cheyne (1777–1836), professor of medicine in Dublin, described chronic hydrocephalus with enlarged head and suture separation; some of his cases, described like Whytt’s as acute hydrocephalus, we can deduce suffered from meningitis:
Pyrexia, with frequent, but short and irregular remissions, flushing, severe headach,…some deeply-seated evil, from the frantic screams and complaints of the head and belly, alternating with stupor, … and vomiting being often brought on by a change of posture.4
At autopsy, he found “the veins of the surface of the brain and lining of the ventricles, gorged with dark blood; sometimes thickening of the membranes, and … ventricles we find to contain from two to six ounces of limpid serum.”
Some of his cases related as “a slow and insidious disease” were probably instances of miliary tuberculosis with tuberculous meningitis:
the surface of the liver studded with small white tubercles, not larger than a grain of mustard. The glands of the mesentery are often diseased, as is evinced by their enlargement, and the caseous depositions which we find in the substance of the glands.
In France, Herpin used the term meningitis in 1803: Méningitis, ou inflammation des membranes de l’encéphale. In England, John Abercrombie (1781–1844) in his textbook5 was one of the first to use the term.
I shall employ the term Meningitis to express the disease, meaning thereby the inflammation of the arachnoid, or pia mater, or both, as distinct from inflammation of the dura mater.
He reported inflammatory pus or cloudy cerebrospinal fluid of the meninges at autopsy. Thereafter the word came into general use.
Gaspard Vieusseux (1746–1814), a Swiss practitioner, reported epidemic meningitis that appeared in January 1805 near Geneva, leading to thirty-three fatal cases in three months.
The popular “miasma theory” of the time attributed the spread of the disease to “bad air” and it was not believed to be contagious. The idea of bacteria causing disease was new. Theodor Klebs, in 1875, was the first to observe bacterial cocci in cerebrospinal fluid (CSF) of patients who died from meningitis. (He also discovered with Friedrich Loeffler the bacterium that causes diphtheria, the Klebs–Loeffler bacillus.)
But it was not until 1887 that Austrian pathologist Anton Weichselbaum identified Neisseria meningitidis (meningococcus, which he named Diplococcus intracellularis meningitides)6 that it was established as the most common cause of cerebrospinal meningitis.7 In 1896, Heubner also discovered meningococci in the CSF of a case of meningitis.8

Several organisms causing meningitis were identified in the late nineteenth century, including Neisseria meningitidis, Streptococcus pneumoniae, Haemophilus influenzae, and Mycobacterium tuberculosis. Thomas Clifford Allbutt in his System of Medicine (1899, vol. VII. 546) gave its clinical context: “In most cases not due to injury meningitis is caused by an invasion of micro-organisms.”
Physical signs of meningeal irritation were described by Vladimir Kernig (1840–1917) and Josef Brudzinski (1874–1917) respectively in 1882 and 1909.9 Examination of the cerebrospinal fluid was necessary for accurate diagnosis. To achieve this, Heinrich Irenaeus Quincke (1842–1922) reported his first lumbar puncture on a patient with suspected meningitis to the Tenth Congress of Internal Medicine at Wiesbaden in April 1891.10 One month later, Walter Essex Wynter reported in the Lancet four children with meningitis: three were tuberculous. He made a small incision into the dura at L2, then inserted a Southey’s tube to withdraw the infected fluid and to reduce the pressure.11
Prevention and treatment
In 1905–6, Simon Flexner,12 von Wasserman, Kolle, and Jochmann began to use intrathecal anti-meningococcal serum therapy to prevent meningococcal disease. This heralded a lengthy chronicle of variable successes interleaved with failures. Injection of horse antiserum into the cerebrospinal fluid became the main preventive measure and therapy. In the First World War, it saved many lives: mortality rates fell from 60–80% to 30–40%.
Schwentker and colleagues introduced sulfanilamide in meningococcal meningitis; ten of eleven patients survived.13 Subsequently, sulphonamides resulted in much improved treatment.14,15 They were cheaper with fewer side effects than the antiserum, although bacterial resistance slowly emerged. By the late 1930s, sulphonamides were the treatment of choice. In the next decade, antiserum and sulphonamides were replaced by benzylpenicillin, which if given urgently proved more effective.16
During World War II, several breakouts in the US Army and civilian populations were successfully treated with penicillin. Subsequent bacterial resistance, a continuing problem, led to the use of other antibiotics and vaccines in current use. Despite them, mortality rates remain at 5 to 10 percent.
References
- Vigon J. transl by Bartholomew Traheron, The most excellent workes of chirurgerye. 1543.
- Whytt R. Observations on the dropsy in the brain. Edinburgh: Balfour, Auld, & Smellie, 1768.
- Cheyne J. Essay on Hydrocephalus Acutus; or Dropsy of the Brain. Edinburgh: Svo. 1808, 218.
- Abercrombie J. Pathological and practical researches on diseases of the brain and the spinal cord. Edinburgh: Waugh and Innes, 1828.
- Weichselbaum A. Ueber die Aetiologie der akuten Meningitis cerebrospinalis. Fortschr Med. 1887;5:573-83. 620-26.
- Osler W, Ledingham JCG. Discussion on the epidemiology of cerebro-spinal meningitis. Lancet. 1915;1:553-5.
- Heubner JOL. Beobachtungen und versuche über den meningokokkus intracellularis (Weichselbaum-Jaeger) Jb Kinderheilk. 1896;43:1-22.
- Pearce JMS. The signs of Kernig and Brudzinski. J Neurol Neurosurg Psychiatry 1992;55:1141.
- Quincke HI. Ueber hydrocephalus. Verhandlung des Congress Innere medizin (X), 1891; 321-39.
- Wynter WE. Four cases of tubercular meningitis in which paracentesis of the theca vertebralis was performed for relief of fluid pressure. Lancet. 1891;3531:981-2.
- Flexner S. Experimental cerebrospinal meningitis and its serum treatment. JAMA. 1906;47:560-6.
- Schwentker FF, Gelman S, Long PH. The treatment of meningococcic meningitis with sulfanilamide. Preliminary report. JAMA 1937; 108: 1407-8.
- De Wardener MK. Sulphanilamide in the Treatment of Meningococcal Meningitis. The Lancet 1937;229:253-5.
- Beeson PB, Westerman E. Cerebrospinal fever. Analysis of 3575 cases, with special reference to sulphonamide therapy. British Medical Journal 1943;1:497-504.
- Meads M, Harris HW, Samper BA, Finland M. Treatment of meningococcal meningitis with penicillin. New Engl J Med. 1944;231:509-17.
JMS PEARCE is a retired neurologist and author with a particular interest in the history of medicine and science.