
JMS Pearce
Hull, England
All the features that characterize Asperger’s syndrome can be found in varying degrees in the normal population.
—JK Wing, Asperger’s syndrome: a clinical account”
Impairment in social interaction, communication, and repetitive and stereotyped behavior characterize autism spectrum disorder (ASD). The prevalence of Kanner’s autism and Asperger’s syndrome—now grouped as ASD—has apparently increased alarmingly in recent decades.1 In 2009, a reputable article claimed a prevalence of 157 per 10,000 children in the UK.2 The US Centers for Disease Control currently states autism affects an estimated 1 in 36 children and 1 in 45 adults in the United States. This provokes the question: has the incidence increased, or have diagnostic criteria widened? Are the so-called characteristics of ASD abnormal, or are they perhaps in some people no more than variations of normal, conventional behavior?
Diagnostic criteria3 are subjective and variable. Wing rightly commented:
As with any psychiatric syndrome identifiable only from a pattern of observable behavior, there are difficulties in determining which are essential for diagnosis. Variations occur from person to person and it is rare to find, in any one case, all the details listed below.4
Autism has been linked to male gender and to a variety of genetic, neurological, and environmental variables, but both neuropathology5 and mechanism(s) remain undetermined and there are no objective diagnostic investigations. The commonly reported comorbidities (gastrointestinal symptoms, developmental disabilities, learning difficulties, obsessive-compulsive behavior, sleep disorders, Tourette syndrome, attention deficit hyperactivity disorder,6 anxiety disorders, social communication disorders) only blur exact definition. In those with developmental disabilities, subtle neurological signs are common: learning difficulties, an increased incidence of epilepsy, viral infections, tuberous sclerosis, fragile X-syndrome.7 In such cases, these factors commonly reflect underlying perinatal organic brain disease, in which autism is symptomatic rather than independent. This is the more severe end of the autistic spectrum.
Many carrying the diagnosis of ASD have been labeled by laymen, self-diagnosed sufferers, or non-medical people: when inaccurate, the result is a false increase in the perceived prevalence. Crucially, diagnosis depends on ideas of what is or is not “normal,” an impossibly vague criterion of widely diverse, traditional, social, and cultural values. The media often exaggerate autistics with enhanced perceptual functioning and special abilities—idiots savants. Draaisma wrote: “in quite a few cases, media representations of talent and special abilities can be said to have contributed to a harmful divergence between the general image of autism and the clinical reality of the autistic condition.”8 There is evidence that such labeling leads to negative medical stereotyping.
The British ASD Clinic states, “There is no cure or specific treatment that works best for individuals with Asperger Syndrome.” Yet some diagnosed with ASD find some sort of relief or respectability in having an identifying medical label. By contrast, many refute the notion that their autism is a disease or disorder and oppose the medicalized model. Similarly, many high achievers with autism view it as a form of “neurodiversity” rather than abnormality. They argue convincingly that diversity in human cognition is normal, and that so-called autistic differences are not necessarily pathological.9
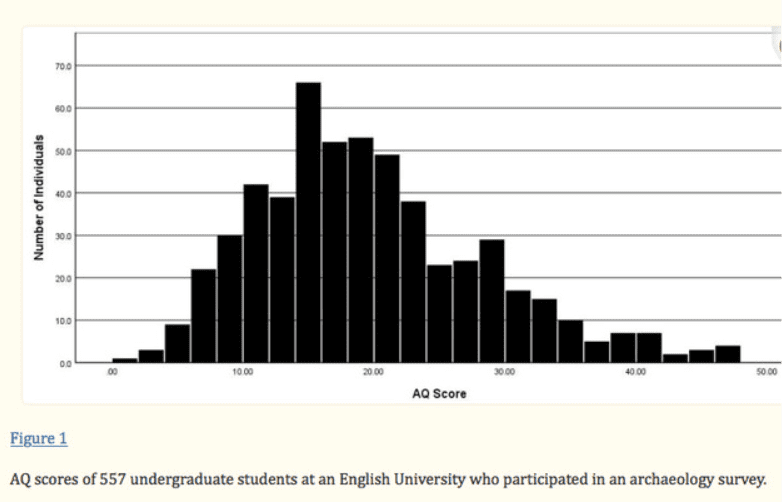
Autism traditionally was considered a clinical condition distinct from the general population, but Baron-Cohen, a leading developmental psychopathologist, has adduced impressive evidence that shows autistic traits are continuously distributed across the population. A sample of 557 university students in the North of England completed an Asperger Questionnaire (AQ). Interestingly, it showed a continuous variation10 in line with large population studies.11 The AQ is not diagnostic; it identifies the extent of autistic traits. These studies confirm that the symptoms ascribed to autism are common across society, a continuum from autism to normality.10,12 Excluding those with objective evidence of cerebral illness, we can reasonably conclude that autistic difficulties of social interaction, verbal communication, heightened or diminished sensitivity to sensory stimuli, and repetitive behavior follow a normal distribution curve across the population.
A high Autism-Spectrum Quotient score does not mean an individual has ASD, since Baron-Cohen insists that the diagnosis is only merited if the individual is suffering a clinical level of distress because of their autistic traits.10 This is supported by the DSM-5 diagnostic criterion (D):
[ASD] Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
Oliver Sacks diagnosed Asperger’s syndrome in the illustrious scientist Henry Cavendish.13 Baron-Cohen suggested that Einstein, too, had Asperger’s syndrome. Professor Michael Fitzgerald, child psychiatrist in Dublin, reported Charles Darwin, with his extraordinary attention to detail but difficulties with social interaction, was probably suffering from Asperger’s syndrome.
These diagnoses have been regarded as retrospective, therefore at best of questionable validity.14 Baron-Cohen did, however, prove that ASD need not be an obstacle to the highest achievements in mathematics, science, and doubtless other careers (Table 1).
Although there is no doubt of the existence of people with autistic features, in ASD there are:
- No specific diagnostic symptoms or physical signs
- No consistent diagnostic abnormalities in laboratory or radiological investigations
- No distinction between the features that characterize ASD syndrome and those found in the normal population10
- Many who are labeled autistic have neither the clinical level of distress, nor significant impairment in social and occupational function necessary for a diagnosis.
Since many diagnosed as autistic fail to conform to suggested criteria and can live and work successfully without conspicuous distress or disability, why have they been medicalized? Have those with unconventional or quirky personalities wrongly been given medical status, and if so, to what purpose? There are children who need support for minor though significant cognitive and learning difficulties caused by various genetic and neurological disorders, whose parents understandably prefer the label of ASD to the stigmata of mental impairment or educational subnormality. More scrupulous application of putative criteria would exclude a large number of people currently diagnosed with ASD, without negating their symptoms.
Wide variations of normal personality, eccentricity, quirkiness, and unconventional behavior indicate the heterogeneity of almost all aspects of autism so that for many, ASD is no more than a group of genuine aberrations of normality, not a valid diagnostic entity but a syndromic description.15 The more severe autistics may be dependent on others and have difficulties in everyday life. They need opportunities and support more than they need treatment.16
Autism and ASD have become overused as socially respectable, medicalized labels for normal if unconventional variations of personality, social behavior, and communication that can embellish the range of humanity and behavior.
Medicalized labeling can also be perilous. A worrying recent suggestion is that those with autism are more vulnerable to grooming and to the radicalization of terrorism. The Financial Times 17 October 2024 reports estimates obtained from psychiatrists working with counter-terrorism police, suggesting the people with autism account for about 13 per cent of their casework against a population base-rate of 1 percent:

Historical note
In 1943 Leo Kanner, a pediatric psychiatrist at Johns Hopkins, recognized eleven children with similar characteristics of innate “extreme aloneness” which he named early infantile autism. In most cases the child’s behavior was considered abnormal from early infancy. Kanner’s more severe autistic patients showed impaired speech, large heads, and motor incoordination.17 Noting a parental influence, he suggested an inborn genetic defect. A year later, Hans Asperger described less severe symptoms of “autistic psychopathy” in eleven young boys of normal intelligence and language development, interests, and activities. Clearly, he said, “It is possible to consider such individuals both as child prodigies and as imbeciles with equal justification.” He also noted cases where an organic disorder could result in a picture that, in numerous critical points, was similar to the picture presented by autistic personality disorder of constitutional origin, stating, “Characteristic stereotypies in particular were common to both the autistic and the brain-injured retarded child.”18 Essential features recounted above are common to Kanner’s and Asperger’s syndromes.
In England, Lorna Wing, co-founder of the National Autistic Society, in 1981 suggested that the term Asperger’s syndrome be used for children and adults; she included thirty-four patients with a wide group of conditions, which had in common impairment of development of social interaction, communication, and imagination. She reported problems of adjustment or superimposed psychiatric illnesses.4 Like Kanner, she described their personalities as “schizoid.” Slightly less than half of Wing’s more typical cases of Asperger’s syndrome were walking at the usual age, but were slow to talk. Ninety percent of Asperger’s cases were poor at games involving motor skills, and sometimes other executive problems. This confirms that at the more severe end of the spectrum lies an underlying organic brain disorder that should be recognized in its own right.
End note
* The criteria for these citations are arguable and inevitably subjective.
References
- Wing L, Potter D. The epidemiology of autistic spectrum disorders: is the prevalence rising? Ment Retard Dev Disabil Res Rev. 2002;8 (3): 151-61.
- Baron-Cohen S, Scott F. J, Allison C, Williams J, Bolton P, Matthews FE, Brayne C. Prevalence of autism-spectrum conditions: UK school-based population study. Br J Psychiatry 2009;194(6):500-9.
- American Psychological Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5) 5th ed. Washington, DC: American Psychiatric Pub, 2013.
- Wing L. Asperger’s syndrome: A clinical account. Psychological Medicine 1981; 11:115-29.
- Haar S, Berman S, Behrmann M, Dinstein I. Anatomical Abnormalities in Autism? Cereb Cortex. 2016;26(4):1440-52.
- Leitner Y. The co-occurrence of autism and attention deficit hyperactivity disorder in children – what do we know? Front. Hum. Neurosci. Sec. Brain Health and Clinical Neuroscience. 2014;8:268.
- Lobascher ME, Kingerlee PE, Gubbay SS. Childhood autism: an investigation of aetiological factors in twenty-five cases. Br J Psychiatry. 1970;117:525-529.
- Draaisma D. Stereotypes of autism. Phil. Trans. R. Soc. 2009 B364:1475-80.
- Pickard C, Pickard B, Bonsall C. Autistic spectrum disorder in prehistory. Camb. Archaeol. J. 2011;21:357-64.
- Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E. The autism-spectrum quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J. Autism Dev. Disord. 2001;31:5-17.
- Ruzich E, Allison C, Smith P, Watson P, Auyeung B, Ring H, Baron-Cohen S. Measuring autistic traits in the general population: A systematic review of the Autism-Spectrum Quotient (AQ) in a nonclinical population sample of 6900 typical adult males and females. Mol. Autism. 2015;6:2.
- Wright B, Spikins P, Pearson H. Should Autism Spectrum Conditions Be Characterised in a More Positive Way in Our Modern World? Medicina. 2020; 56(5):233.
- Sacks O. Uncle Tungsten: Memories of a Chemical Boyhood. Vintage Books, 2001.
- Jungnickel C, McCormmach R. Cavendish. In: Cavendish: The Experimental Life (2nd edition), Berlin: Max-Planck-Gesellschaft zur Förderung der Wissenschaften, 2016.
- Pearce JMS. Disease, diagnosis or syndrome? Practical Neurology 2011;11: 91-7.
- Mottron L. The power of autism. Nature 2011;479:33-5.
- Kenner L. Autistic disturbances of affective contact. Nervous Child: Journal of Psychopathology, Psychotherapy, Mental Hygiene, and Guidance of the Child 1943;2:217-250.
- Asperger H. Die ‘Autistischen Psychopathen’ im Kindesalter. Arch fur Psychiatr Nervenkr 1944;117:76-136.
JMS PEARCE is a retired neurologist and author with a particular interest in the history of medicine and science.