
Jonathan Davidson
Durham, North Carolina, United States
The Civil War between the States took a heavy toll, claiming over 600,000 lives, or two percent of the population. Countless more suffered from injuries and other diseases. Reilly1 has listed some of the advances in medical care that took place during this conflict. For the most part, the Northern states were better positioned, since resources were poor in the Confederacy. Furthermore, most Confederate war records were destroyed by fire at the end of hostilities, leaving much unknown. Despite an uphill struggle to organize and provide adequate care in the South, three physicians were conspicuous for their work and impact on overall healthcare.
Samuel P. Moore
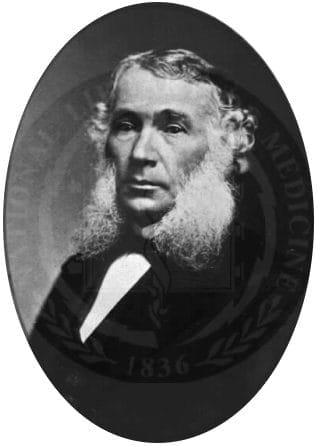
Samuel Moore2 (1813–1889, Figure 1) was born in Charleston, South Carolina and received his medical education at the South Carolina Medical College (now Medical University of South Carolina). In 1834 he moved to Little Rock to open a medical practice, but the next year joined the US military as an assistant surgeon, serving variously on the frontier, in the Mexican-American War, and the US Military Academy at West Point. It was during service in the Mexican-American War that Moore met and became friends with Jefferson Davis. After secession of the Southern states, Davis appointed Moore to the post of surgeon-general in 1861, where he remained until 1865.
Moore faced many obstacles in establishing a medical department yet achieved notable successes. Faced with a serious shortage of trained doctors, he created a two-step training program, at the end of which doctors who had failed a preliminary exam either took and passed an exam or, if they failed again, were removed from service. By the end of the war, Moore’s department had recruited 3,000 people. Beyond this was Moore’s ability to mold together a group of opinionated doctors to follow a common set of practice standards. In building his department, one innovation was to include dentists in the medical corps. Dental health was not good, and soldiers were often missing teeth. As it was necessary to bite into rifle cartridges to access powder, a set of front teeth was essential. (Use of the phrase “4F” derived from this time, referring to soldiers who had four missing front teeth and were graded as unfit for duty.)
Medicine and supply shortages were problematic, exacerbated by the Union blockade of Southern ports. To rectify this, Moore set up laboratories to manufacture drugs from indigenous plants and surgical instruments that were sometimes based on designs of captured materials from Northern troops. Moore also appointed trained professionals to research medications and other aspects of healthcare.
To promote communication between medical professionals, Moore started the Confederate States Medical and Surgical Journal in 1864, a widely read and well-respected publication edited by James McCaw (see below). A shortage of paper at the end of the war lead to its demise. As a companion, Moore also updated Chisholm’s Manual of Military Surgery in 1864, to very favorable reviews in the press. To promote meetings and exchange of information, Moore established in 1863 the Association of Army and Navy Surgeons of the Confederate States of America, believed to be the first medical society in the US.
Arguably, and of greatest consequence, was Moore’s establishment of Chimborazo Hospital in Richmond in 1861.3 Its design and overall record of success may have been responsible for changing the attitude of the American public and medical professionals towards hospitals, which had been associated with terminal illness, death, and social isolation: places to be avoided at all costs. Moore modeled Chimborazo to a degree on the medieval Knights Hospitaller hospitals. Chimborazo consisted of five divisions of thirty buildings each, accommodating 3,000 patients. Each ward had 20–40 beds grouped according to disease. The barracks-style pavilions were well-ventilated and separated by wide avenues. In addition, the hospital had a bakery, brewery, ice houses, soup kitchens, bathhouses, and pastures for cattle and goats. Visits and gifts of food or clothes were welcomed. Chimborazo was a model for military hospital design for many subsequent decades and a beacon for changing attitudes towards hospitals. It has been said that Moore provided “discipline, leadership and calm in the midst of turmoil and trouble.”3 In total, 78,000 patients passed through Chimborazo, where the mortality rate was 9%, slightly lower than in Union hospitals.
After the end of hostilities, Moore took the oath of allegiance and retired to Richmond, where he was active in public education and a well-respected member of the community.
James B. McCaw
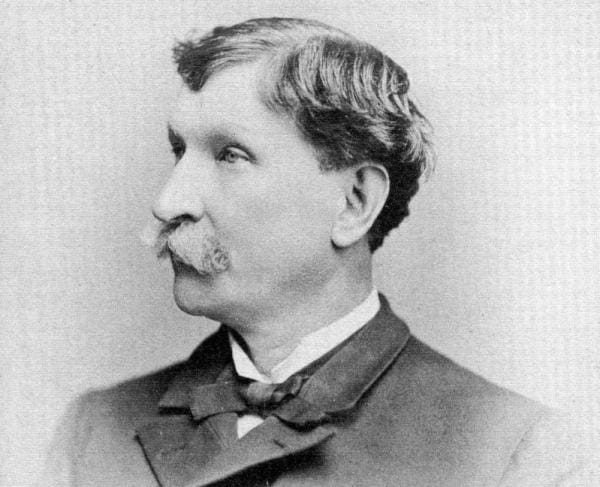
James McCaw (1826–1906, Figure 2) came from a line of well-established doctors in Richmond, Virginia.4 In 1844, he graduated from the Medical College of New York University and returned to his hometown, where he set up medical practice. He also held a faculty position at the Medical College of Virginia (MCV), which was the only Confederate medical school to stay open throughout the war. As chief editor of the Confederate States Medical and Surgical Journal, an academic, and a clinician, he remained aware of medical advances.5 Early in the war, after the Battle of Bull Run, McCaw was chosen by Samuel Moore to become surgeon in charge of the new Chimborazo Hospital, an ideal choice that reflected on McCaw’s leadership skills. He reported only to the Confederate Medical Department and had a largely free hand in running the hospital. He was responsible for hiring and training, administering medical care, and promoting harmonious relationships among the staff. It was said by one of the matrons that “difficulties melted away beneath the warmth of his ready interest.” After the war ended, McCaw became president and dean of MCV and served on the board of directors. He died in 1906.
Joseph Jones
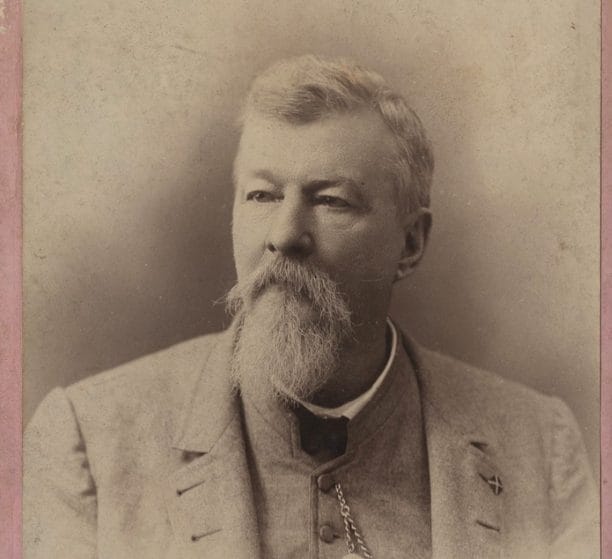
Moore had a talent for finding competent professionals to whom he could delegate, one of whom was Joseph Jones (1833–1896, Figure 3). Jones was born in Georgia and studied medicine at the University of Pennsylvania, graduating in 1856. He then served on the faculties of the Savannah Medical College, Medical College of Georgia, University of Nashville, and Tulane University. Among his varied interests were medical education, public health and quarantine rules, clinical and laboratory research, epidemiology, and archaeology.
At the beginning of the war, Jones enrolled in the army as a private and was then appointed by Moore to a surgeon position, which allowed him to pursue research related to diseases and injuries associated with battle and captivity. He became known as “one of the most outstanding Confederate medical officers of the American Civil War.”6 He described so-called “hospital gangrene” (necrotizing fasciitis) and contributed to the post-war US Sanitary Commission Report by giving a clear and modern description of the condition. To prevent it, he suggested cleanliness, dietary measures, and ventilation. For systemic treatment he advised mercury purges, iron tonics, quinine, turpentine oil, and opiates. For local therapy he advocated nitric acid, camphor, and creosote. It should be remembered that these ideas were expressed before germ theory and antisepsis were introduced to medicine.
Other contributions included over 100 publications, extensive memoirs, the identification of the typhoid bacillus and malaria plasmodium, and descriptions of the horrific conditions at the Andersonville prison camp with proposals for amelioration. For malaria, he proposed alternative treatments to quinine, which was in scarce supply, and he worked to develop Epsom and Glauber’s salts.7
After the war ended, Jones returned to Nashville as a health officer before moving to Tulane in New Orleans, where he remained for rest of his life. In 1870 he published an article based on his archeological excavations in Nashville, which demonstrated that the city was built on a burial ground for pre-Columbian natives. He described bone evidence of syphilis, the first known paleopathological report of its type by a medical professional. Between 1880–1884, Jones was president of the Louisiana Board of Health, where he fought to preserve states’ rights over federal control of public health issues. After the National Board of Health closed in 1873, Jones returned to academic life at Tulane.
In conclusion, it is clear there were great challenges in providing medical care in the Southern US states between 1861 and 1865. This did not prevent innovations or good leadership by physicians such as Samuel P. Moore, James B. McCaw, and Joseph Jones.
References
- RF Reilly. “Medical and surgical care during the American Civil War, 1861-1865.” Proc Bayl Univ Med Cent. 2016; 29(2):138-142.
- PN Purcell, RP Hummel. “Samuel Preston Moore: Surgeon-General of the Confederacy.” Am J Surgery. 1992; 164: 361-365.
- CE Bagwell. “Nosokomia to sacred infirmary: Legacy of the Knights Hospitaller and Chimborazo Hospital in the evolution of hospitals from medieval to modern.” 2013. J Am College Surgeons 216(4):p e35-e42, April 2013. http://dx.doi.org/10.1016/j.jamcollsurg.2013.01.001.
- “Dr. James B. McCaw,” from The Virginia Magazine of History and Biography. 1954; 62(2): 190-200. Accessed at https://www.nps.gov/rich/learn/historyculture/dr-james-mccaw.htm. August 18, 2024.
- CC Green. Chimborazo: The Confederacy’s Largest Hospital. Knoxville: University of Tennessee Press, 2004, page 22.
- WF Quirk, Sternbach G. “Joseph Jones: Infection with flesh eating bacteria.” J Emergency Med. 1996; 14(6): 747-753.
- JO Breeden. “Joseph Jones and Confederate medical history.” Georgia Hist Q. 1970; 54(3): 357-380.
JONATHAN DAVIDSON received his medical and psychiatric training at University College Hospital, London, and the Royal Edinburgh Hospital, Edinburgh. He practiced psychiatry at Duke University, and has published articles on psychopharmacology and medical history.
One response
A terrific paper, among the many you have written over the years! These medical leaders in the South and their methods evoke many items in my memory, some of which might be wrong after this long. I recall reading that the Civil War was the worst war that America has ever seen. There are several reasons beginning with how large the number of combatants were involved. Also, hospitals were distrusted, there were no antibiotics, fluid replacement and wound care were rudimentary, etc.
My great, great grandfather fought for the North in the Cavalry. His horse was shot out from under him, so he got an early discharge. However, he became an Alcoholic. He quit alcohol apparently because so many people were telling him it was going to kill him. His wife and children lived ever so much better thereafter.
My father, a corporal in WWII was wounded, but happily survived. They were 17 flesh wounds from shrapnel. He laid as if dead because there were German snipers in the trees. When smoke came along, he got up and limped to the nearest aid station. He was sent to England where the wounds were debrided and closed. I still have his handkerchief with holes in it and blood stains. I also have his Purple Heart. For at least 15 years after the war, he was a local hero. He would march in the local Memorial Day parade; He used his G.I. Bill to finance a 4-year apprenticeship to become a master plumber. We still have his plumbing truck, which was broken down and damaged in a garage fire. I spent $34,000 restoring it, and it still appears in parades.
A salute to you and to that venerable British Prime minister – Winston Churchill. THANK YOU!!!