
Howard Fischer
Uppsala, Sweden
“By consistently tormenting them / with reminders of the lice in their children’s hair, the / School Physician first brought their hatred down on him / But by this familiarity they grew used to him, and, so / at last, they took him for their friend and adviser.”
—“The Poor,” William Carlos Williams, MD
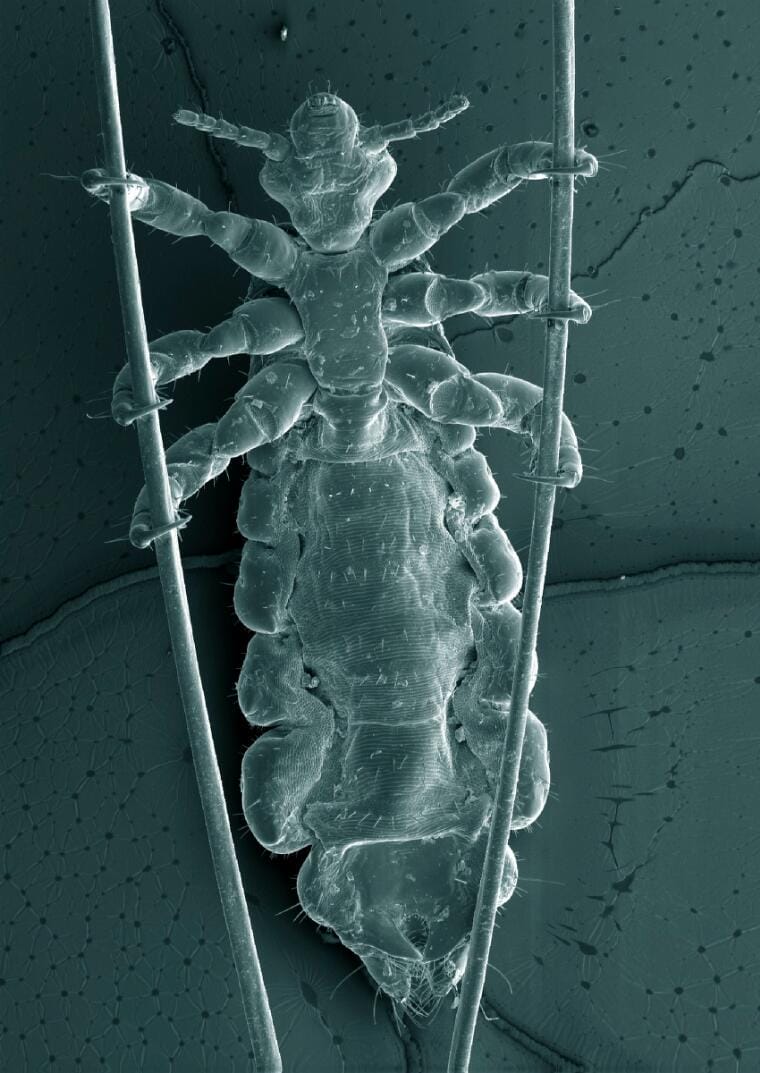
There are between six and twelve million cases of head lice annually in the US. Head lice (Pediculus humanus var. capitis), unlike body lice, do not transmit any systemic diseases. Lice are wingless insects 1–4 mm in length—about the size of a sesame seed. They crawl and climb, but neither jump nor fly.1 Close contact and fomites such as hats, helmets, headphones, scarves, and combs and brushes are the means of transmission of head lice.2 They lay eggs on hair shafts, close to the scalp surface, especially in the occipital area and above the ears. The eggs hatch in seven to ten days. These insects feed by piercing the skin surface, injecting anticoagulant-containing saliva, and sucking the blood. Lice live three to four weeks and cannot survive more than two days away from their human host. Children from three to twelve years of age are most commonly infested, girls more often than boys. All socioeconomic groups may be affected; the presence of head lice is not an indication of lack of hygiene or cleanliness.3 The adult insect maintains its position on the hair shaft by means of its six claws, each one attached to one of its legs.
The louse “knows” that “all hair is not alike.” In cross-section, the shaft of white, Asian, and Native American hair is round. That of African and African American hair is oval. The lice that predominate in the US came with early white settlers and can only grip hair shafts with a round cross-section. Black children are rarely infected with head lice in the US.4-12 Prevalence estimates are “probably less than one per cent” in Black school children,13 perhaps even less than 0.5%.14 A countywide study of elementary school children in Florida15 detected head lice in 6.4% of 1,515 Hispanic, Asian, and white children, and no head lice in 436 Black children.
In addition to the widely held belief that the hair shaft shape hinders lice with European ancestry from grasping the hair of African Americans, it is suggested that use of hair products at a younger age16 and type of preparation17 may make the “hair environment less friendly for the louse and more difficult for it to obtain a satisfactory meal and lay its eggs.”18
This writer (HF) trained, practiced, and taught pediatrics in an inner-city university hospital for forty-five years, in a city with an 80% Black population. He never saw head lice in a Black child, and neither had the colleagues he questioned. The authors of a study from New York City this year state that their work “dispels the myth that Black children cannot get head lice.” Of 254 children diagnosed with head lice in the study, 15% were Black.19 These results need replication from other centers.
Head lice may be treated with a variety of topical medications, as well as some oral medications for resistant cases. While this is a condition without medical consequences—apart from the occasional secondary infection—it is associated with disgust, anxiety, embarrassment, time spent away from school, and days off work for parents, as well as the cost of treatment.20
References
- Sherman Alter et al. “Common child and adolescent cutaneous infestations and fungal infections,” Curr Prob Pediatr Adolesc Health Care 48(1), 2018.
- Walter Pray. “Head lice: Perfectly adapted human predators,” Am J Pharmaceutical Education 63(2), 1999.
- Alter, “Common infestations.”
- Alter, “Common infestations.”
- Pray, “Head lice.”
- Eugenia Shmidt and Lacob Levitt. “Dermatologic infestations,” Int J Dermatology 51(2), 2012.
- Constance Mazurek and Nancy Lee. “How to manage head lice,” West J Med 172(5), 2000.
- Beth Sissons. “Head lice and coily hair: Signs and treatment,” Medical News Today, October 29, 2021.
- “Head lice. Epidemiology & risk factors,” CDC, 2019.
- I. Nutanson et al. “Pediculus humanus capitis: An update,”Acta Dermatovenerol Alp Pannonica Adriat 17(4), 2008.
- Patricia Sciscione and Cheryl Krause-Parello. “No-nit policies in schools: Time for change,” J School Nursing 23(1), 2007.
- Suzanne Pinto. “Bites: Head lice,” Journal for Specialists in Pediatric Nursing 11(2), 2006.
- Joan DiNapoli et al. “Eradication of head lice with a single treatment,” AJPH 78(8), 1988.
- Sissons, “Coily hair.”
- W. Price and Amparo Benitez. “Infestation and epidemiology of head lice in elementary schools in Hillsborough County, Florida,” Florida Scientist 52(4), 1989.
- Sissons, “Coily hair.”
- Shmidt and Levitt, “Dermatologic.”
- Sciscione and Krause-Parello, “No-nit.”
- McCall Torpey et al. “34998 Racial factors regarding diagnosis and treatment of head lice in pediatric patients” (abstract), Journal of the American Academy of Dermatology 87(3), Supplement, AB99, 2022. https://doi.org/10.1016/j.jaad.2022.06.430.
- Alter, “Common infestations.”
HOWARD FISCHER (1947–2024), M.D., was a professor of pediatrics at Wayne State University School of Medicine, Detroit, Michigan.
Highlighted in Frontispiece Volume 18, Issue 3 – Summer 2026