
JMS Pearce
Hull, England
Clinical MS: Augustus D’Este, McKenzie
It was almost two centuries ago that the best known and possibly the first detailed patient’s description of multiple sclerosis (MS) was recorded. It survives in the diaries (1822-48) and almanac of Sir Augustus D’Este, the Harrovian grandson of King George III.1,2 In December 1822, when he was twenty-eight years old, Augustus suffered impaired vision in both eyes that recovered—probably bilateral optic neuritis. In successive years, he noted progressive weakness, numbness, difficulty in walking, painful spasms, and depression: with hindsight, typical of MS. Although aged fifty-four when he died, no formal diagnosis was made, but “the meticulous notes in his diary justify a posthumous diagnosis.”3
In his treatise De la moelle epiniere et de ses maladies, Paris, 1824, Charles Prosper Ollivier (D’Angers) independently gave another credited clinical description of MS in chapter eight, headed myelitis. The patient was a twenty-year-old notably cheerful man with paresis of his right hand and legs, urinary retention, speech disorder, and a fluctuating course over twenty-nine years after an onset in 1808.
Ian McDonald4 recorded what he said may have been multiple sclerosis subsequent to optic neuritis, which precedes Carswell’s description of its pathology. (Fig 1) In a text written in 1840, William McKenzie had described a twenty-three-year-old man, Thomas Crighton, who:
. . . Was admitted into St. Bartholomew’s Hospital, on account of a palsy of his limbs’, which had evolved progressively over the preceding six months. He had, at the commencement of his illness, ‘. . . a (progressive) confusion of vision (so that) he could discern no object distinctly’. He was incontinent and was developing an asymmetric weakness of the arms and dysarthria. Mr Abernethy treated him with rhubarb, calomel and gentian. After three weeks “. . . he could move his hands and arms nearly as well as ever; and his eyesight was so much improved that he could read a newspaper . . . the functions of the bladder were completely restored; his speech became articulate . . . but with little amendment of the lower extremities.” 5
Previously, physicians had described similar symptoms but failed to synthesize them into an identifiable disease entity.
Pathology of MS: Cruveilhier, Carswell
Jean Cruveilhier (1791–1874) (Fig 2),6 the first professor of pathological anatomy in Paris working in the Charité and Salpêtrière hospitals, is often credited with the first pathological account of multiple sclerosis (MS). He published an atlas in which he illustrated the lesions of sclérose en plaques later known as disseminated (DS) or multiple sclerosis (MS). He first illustrated the lesions in the second volume dated 1835-1841 that contained forty livraisons published in parts, but the pathological lesions of MS did not appear until 1841 in livraison 32 plate 2, and livraison 38 plate 5, both in volume 2, as confirmed by Charcot.

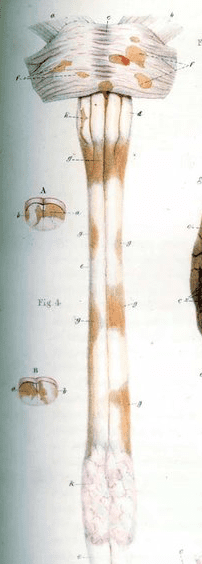
Robert Carswell (1793–1857) (Fig 3) published his Pathological Anatomy; Illustrations of the Elementary Forms of Disease in 1838. His depiction of the lesions of MS7 appears on plate 4 (Fig 1), which therefore predates Cruveilhier’s illustration by at least three years,3 although as a pathologist Carswell never examined his patients in life.
The preface to Carswell’s atlas is dated 15 December 1837, but his cases were observed before 1831.8 His atlas described:
in the section on atrophy is ‘a peculiar diseased state of the chord and pons Varolii, accompanied with atrophy of the discoloured portions . . . the atrophy was more conspicuous in some points than in others. . . . FF Isolated points of the pons Varolii of a yellowish brown colour; GGG. Patches of the same kind on the spinal chord, all of them occupying the medullary substance which was hard, semitransparent and atrophied . . . H affects the right olivary body; K softening of a portion of the chord. Figure 4, A and B . . . cord show that the discolouration commences on the surface of the white and extends into the grey substance.
Trained in Glasgow, Carswell was an “artist–pathologist” who prepared a collection of anatomical drawings for the lectures of an Edinburgh physician. He traveled to Paris and Lyon where during 1822-3 and again in 1826 he compiled hundreds of illustrations of pathological material. In 1826 he obtained the MD from Aberdeen. He was appointed the first professor of pathological anatomy at University College London (1828), worked there as a physician, and later was physician to Leopold I, King of the Belgians. He suffered chronic lung disease, probably tuberculous, and died in 1857.
Clinicopathological correlations: Charcot, Vulpian, and Moxon
The defining clinical features were not adequately recognized until the writings of Alfred Vulpian (1826-1887) and Jean-Martin Charcot (1825-1893) who worked together in La Salpêtrière laboratory. The renowned Charcot introduced the term sclérose en plaques.9 With Vulpian, his lifelong friend, Charcot initially identified clinical features of a spinal form of multiple sclerosis in three patients.10 In 1866 he started his famous formal courses of lectures (Fig 4) on Fridays at La Salpêtrière hospital.

{kind=link}
I will, finally, point your attention to a certain number of affections, which have not yet been completely cleared from the unformed group—the real chaos—of chronic myelitis, and which, pardon me the word, are not yet officially recognized; such are for example the sclerosis of lateral bundles and disseminated sclérose en plaques. (Leçons cliniques, Lecture VI, VII, Charcot)12
Fully acknowledging Vulpian’s work, he gradually provided full clinico-pathological expositions of MS that included periods of remission and relapse.11,12 He distinguished the tremor and incoordination from Parkinson’s paralysis agitans with which it was often confused. He described the lesions in detail, noting relative sparing of axis-cylinders, fatty granulation of myelin, hypertrophy of neuroglia, and the scarring in the plaques. Charcot attributed symptoms to impaired conduction in nervous tissues. He identified a characteristic “Charcot’s triad” of cerebellar symptoms: nystagmus, slurred speech, and ataxic incoordination.
The British were, however, late on the scene. Moxon in 1875 gave an excellent account of eight patients13 but noted:
“The recognition of this disease by English physicians will appear singularly slow . . .”
Astutely, he recognized early remissions and the disseminated distribution of sclerotic patches. He described a conspicuous vessel in the center of a patch, perhaps predicting the later recognition of its immunological features and the importance of the early disruption of the endothelial blood-brain barrier. In 1916, James Dawson of Edinburgh described the pathological importance of inflammation and damage to myelin sheaths (demyelination) of neural tissues with resulting “scarring” in the plaques. Thomas Buzzard’s major review of 1893 related optic neuritis to disseminated sclerosis in five patients who had episodes of visual failure with recovery.14 Uhthoff found six instances of DS in a series of 120 cases of optic neuritis. He noted, “bodily exercise with fatigue caused a marked worsening of vision,” now called Uhthoff’s sign, related to small rises in body temperature.15
The Journal of a Disappointed Man
In the twentieth century came the sad saga of the natural historian Bruce Frederick Cummings (1889-1919), under the pseudonym Wilhelm Nero Pilate Barbellion. He predicted his own demise in his The Journal of a Disappointed Man.16,2 Aged twenty-four, Barbellion first records in his diary that his speech and right side are impaired and mistakenly believes that he must have locomotor ataxy;a he consulted the highly regarded neurologist Henry Head, but not until 1915 did he learn that Head had diagnosed disseminated sclerosis, but communicated this only to his family. Over the next two years Cummings relates further fluctuating symptoms, recognizable as MS. However, rejected when enlisting for service he read on his medical certificate that DS had been diagnosed. He became understandably depressed and dismayed, a state not improved when he consulted the section on DS by Risien Russell in Sir Thomas Allbutt’s System of Medicine; the Histology of Disseminated Sclerosis by JW Dawson; and the writings of Pierre Marie. After remission, he relapsed with increasing weakness of his limbs and paraesthesiae in the hands. Now morbidly introspective, he wrote in his diary (1917):
‘The millions of bacteria gnawing away my precious spinal cord . . . I am not offering up my life willingly – it is being taken from me piece by piece, while I watch the pilfering with lamentable eyes.’
He died, aged thirty in October 1919. His account that contained a preface by HG Wells was at first treated with contempt, though later it was regarded as a minor literary classic.
Not until the 1960s was the theory established that MS is an autoimmune disease, in which the immune system attacks myelin. A comprehensive monograph, Multiple Sclerosis, was written in 1955 by Douglas McAlpine, Nigel Compston, and Charles Lumsden. Alastair Compston and collaborators edited and expanded a fourth edition in 2005.
Endnote
- locomotor ataxia was synonymous with syphilitic tabes dorsalis.
References
- Firth D: The Case of Augustus D’Este. Cambridge, Cambridge University Press 1948.
- Pearce JMS. “Historical descriptions of multiple sclerosis. The stories of Augustus D’Este and the journal of a disappointed man” European Neurology 2005; 54, No. 1, pp. 49 – 53.
- Compston A. The 150th anniversary of the first depiction of the lesions of multiple sclerosis. J Neurol Neurosurg Psychiatry 1988; 51: 1249¬52.
- McDonald WI. Physicians, subsequence and consequence. J Neurol Neurosurg Psychiatry 1999;67:282–289.
- McKenzie W: A Practical Treatise on Diseases of the Eye, Ed 3. London. Longman, 1840. Case 920, p.1070-1.
- Cruveilhier J. L’Anatomie pathologique du corps humain; descriptions avec figures lithographiées et coloriées: diverses alterations morbides dont le corps humain est susceptible. Vol 2; Liv 32, Pl 2, pp. 19–24; Liv 38, Pl 5, pp. 1–4. Paris, Baillière, 1829-42.
- Carswell R. Illustrations of the Elementary Forms of Disease. London: Longman, 1838. Plate 1V fig1.
- Dunea G. Sir Robert Carswell, illustrious medical illustrator. Hektoen International Journal. Summer, 2020
- Zalc B. One hundred and fifty years ago Charcot reported multiple sclerosis as a new neurological disease. Brain. 2018; 141(12): 3482–3488.
- Vulpian A. Note sur la sclérose en plaques de la moelle épinière. Communication à la Société Médicale des Hôpitaux le 9 Mai 1866. Union médicale 1866; 3: 75–100.
- Charcot JM. Histologie de la sclérose en plaques. Gaz Hop (Paris) 1868; 41: 554-4, 557-8, 566.
- Charcot M. Lectures on Diseases of the Nervous System. Translated and edited by George Sigerson. London: The New Sydenham Society, 1877. pp.157-182.
- Moxon W. Eight cases of Insular Sclerosis of the brain and spinal chord. Guy’s Hospital Reports 1875; 20: 437–80
- Buzzard T. Atrophy of the optic nerve as a symptom of chronic disease of the central nervous system. Br Med J 1893; 2:779-784.
- Pearce JMS. Early Observations on Optic Neuritis and Uhthoff’s Sign. Eur Neurol 2010;63:243-247.
- Barbellion WNP. The Journal of a Disappointed Man. London: Chatto and Windus 1919.
JMS PEARCE is a retired neurologist and author with a particular interest in the history of science and medicine.
Highlighted in Frontispiece Volume 13, Issue 2– Spring 2021