
John Hayman
Melbourne, Australia

Tom Wedgwood (1771-1805) was born into the famous pottery dynasty as the third surviving son of Josiah Wedgwood (1730-1795) and his wife Sarah (1734-1815). Sarah was also a Wedgwood, a distant cousin of her husband.1 Tom was ill for all of his short life, a life recorded by his biographer, Richard Litchfield.2 Details of his suffering also come from letters to his father and to his siblings, many transcribed in The Wedgwood Circle.1 Tom was the maternal uncle of Charles Darwin (1809-1882), the famous naturalist, born four years after Tom died.
The first existing mention of Tom’s illness comes in a footnote to a letter written to his father in 1783 from his home, Etruria, when he was twelve years old: “P.S.⏤I would have written this letter well but I have got the head ache, but did not like to miss the opportunity of a box” (boxes of goods dispatched from the pottery works).2 Tom attended Edinburgh University from 1786 to 1788 where he studied natural philosophy and corresponded with Alexander Chisholm, a chemical assistant and secretary working with his father. Josiah and Chisholm both advised Tom to play golf, already popular in Scotland, as a means of avoiding headaches. Tom did not graduate, probably a result of his early health problems.
Back at Etruria, Tom carried out experiments that would influence the development of photography. His paper “Experiments and observations on the production of light from different bodies, by heat and attrition” was read before the Royal Society in December 1791. His scientific endeavors would not last, and in April 1792, shortly before his twenty-first birthday, he wrote: “But not succeeding in my trials at a vacuum, and finding my health impaired, I resolved to give up experimenting.” He suffered from exhaustion, depression, visual disturbances, and headaches so severe that he would sometimes throw himself to the ground screaming.2
Tom tried unsuccessful treatments, some devised by the physician Thomas Beddoes (1760-1801), such as therapy at Beddoes’ Pneumatic Institution in Bristol. Here patients were treated by inhalation of different gases, treatment that Tom predicted and concluded was ineffectual. Tom also tried the “warm-room plan” devised by Beddoes, living in a sealed room heated to 70°F (21°C) for 72 hours.
In February 1800 Tom sailed for the West Indies in the hope that the change in climate would improve his health. He spent most of the seven-week journey in his cabin, suffering seasickness as well as headaches and stomach pains.1 Once ashore his symptoms seemed to improve: “I gain strength very rapidly. . . . If I had no indigestion and headache I should be in heaven . . .” This improvement, if improvement it was, did not last and by June he was back in England. Headache was his most disabling symptom, but he also had abdominal pain, depression and anxiety, and a continuing restlessness.
Tom had been introduced to opium by the poet Samuel Coleridge (1772-1834), whom he had befriended and supported. He was preparing for another trip to the West Indies when he died. “Bessy” (Elizabeth, née Allen 1764–1846), his brother Josiah’s wife, wrote to her sister Emma Allen (1780-1866): “. . . on Monday I think he got a little chilled, which brought on much internal pain, and left him weak . . . at midnight he rang his bell, and told his servant to give him something, for he was very weak, but not ill. He told him also to come in in two hours’ time, and see how he was, and to call Jos at five. The servant did so, and found him as he thought sleeping, but in fact he was then without any sign of sense except that he still breathed.”2 His brother stayed with him for twelve hours until he died. Bessy added: “I quite feel it a blessing to us and to him that he died now, before he went aboard-ship, rather than to have suffered all the pain of parting and then perhaps to have sunk under the first attack of seasickness, which I now suppose would certainly have been the case.” Tom’s death was clearly expected; he died without pain and almost certainly assisted by opium.

Tom’s illness would today probably be diagnosed as abdominal migraine, a condition mostly of children but which may persist into adult life and is associated with classical migraine.3 Examination of his family history provides information as to a possible intrinsic cause of his illness. Susannah (‘Sukey’ 1765-1817), the eldest child, married Dr. Robert Darwin and was Charles Darwin’s mother. She was chronically unwell—“everyone seems young but me”—with arthritis and probable hyperemesis with pregnancies.4 She died from an acute abdominal condition with peritonitis—possibly acute pancreatitis. John (1766-1844), the eldest son, suffered with tremor all his life. The third child, Richard (‘Dicky’ 1767-68), died suddenly at ten months. Josiah II developed Parkinson’s disease in later life.
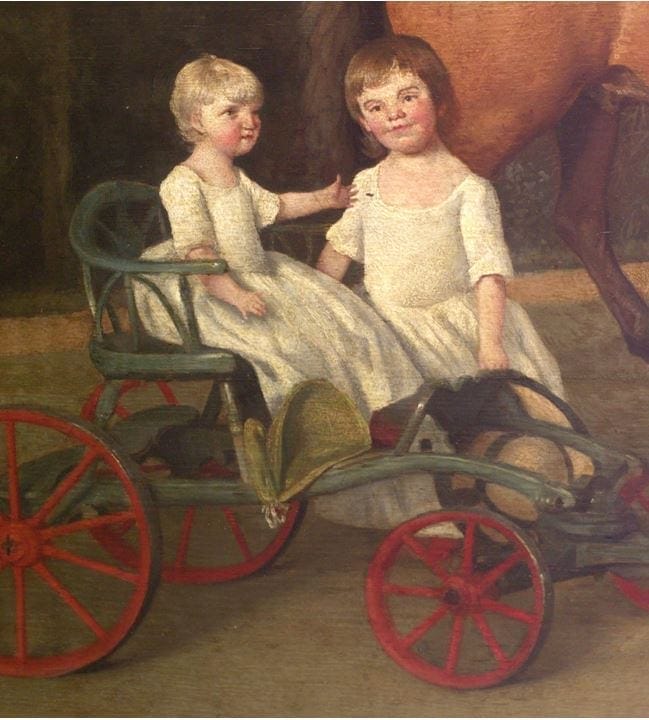
The child after Tom was Catherine (‘Kitty’ 1774-1823), described as having a masculine appearance and never married. In later life she developed an abdominal tumor that reached to an immense size. Her masculine appearance suggests she may have had polycystic ovary (Stein-Leventhal) syndrome, the commonest cause of such endocrine effects in females.5 Cystic tumors develop in this condition, which if untreated may become massive. Sarah (1776-1856) had no history of illness, but in the portrait of the family (Figures 2, 3) she is depicted as having eyes set wide apart (ocular hypertelorism).
The youngest child of that generation, Mary Ann (1778–86), was born with short stature, was physically and mentally impaired, and suffered seizures with episodes of blindness.6 Despite treatment by Josiah’s friend, Dr. Erasmus Darwin (1731-1802), she deteriorated and died at the age of eight. In the family portrait, the artist Stubbs, with his eye for detail, has depicted her in a cart being partly supported by Sarah, suggesting that she could not walk or even sit upright without support. The unusual shape to her dress suggests that she is wearing incontinence padding. She has hands with short fingers (brachydactylia). Mary Ann had characteristic features of the MELAS (Mitochondrial myopathy, Encephalopathy, Lactic acidosis, Stroke-like episodes) syndrome, one of the first recognized mitochondrial disorders.7
The mother of this generation, also named Sarah, although living to old age, was chronically unwell, having arthritis and symptoms that today would be described as consistent with fibromyalgia.8 Between the birth of Tom and Catherine she suffered a spontaneous abortion and became severely ill from what Dr. Darwin called “inflammation of the liver,” possibly acute fatty liver of pregnancy. This constellation of symptoms suggests that Sarah may have had a mitochondrial DNA (mtDNA) mutation that was passed to her son Tom and to her other children.
Mitochondria are cell organelles that produce most of a cell’s energy requirements. Their numbers in a cell vary from a hundred to thousands, depending on energy requirements.9 Unlike other organelles they contain their own DNA, mtDNA. Like nuclear DNA, mtDNA may undergo mutation, potentially impairing mitochondrial function. Mitochondria with mutant DNA coexist with fully functional mitochondria, a condition referred to as heteroplasmy. When a cell divides, mitochondria flow randomly to daughter cells so that these may differ in their level of heteroplasmy.
Ova contain several thousand mitochondria and ova from the same mother may differ considerably in their level of heteroplasmy. Mitochondrial disease, unlike genetic disease due to nuclear DNA, does not relate to the type of mutation but rather to the level of heteroplasmy of the ovum and the subsequent random distribution of mutant mtDNA in the tissues of the embryo. Thus, the one mutation may produce very different clinical disorders in descendants from the same mother.10
As well as MELAS, pathogenic mtDNA mutations have been shown to be responsible for other neurological conditions such as migraine type headaches,11 visual disturbances, Parkinson’s disease, other tremors, and susceptibility to motion sickness.10 Psychiatric symptoms include depression and anxiety;12 lethargy is also common. Skeletal abnormalities such as bradydactyly and hyperteleorism also occur,13 as does abdominal and muscle pain, and pancreatitis is a recognized complication.14 In females mtDNA mutation has been shown to be associated with polycystic ovaries with subsequent cystic tumors;15 spontaneous abortions may occur in pregnancy. Acute fatty liver is recognized as a complication of both mitochondrial disease and pregnancy.16
A pathogenic mtDNA mutation affecting cells with high metabolic requirements such as cerebral endothelial cells would explain Tom Wedgwood’s illness with his excruciating headaches and visual disturbances. The same mutation with different heteroplasmy levels and tissue distribution may explain the whole range of illnesses that affected his mother and the other children of that Wedgwood generation. Through Susannah, the oldest child, the next generation would have received the same errant mtDNA.
Tom’s illness had similarities to that of his famous nephew, Charles Darwin, who was Susannah’s second son, born four years after Tom’s death. Both suffered from persistent seasickness, headaches, abdominal pain, lethargy, and anxiety—both have been diagnosed as suffering from hypochondriasis.1, 17 Such similarity is not surprising if the nature of Tom’s illness is correct. Both Tom and Charles would have received the same mutant mtDNA from their respective mothers. Charles Darwin’s illness saved him from “the distractions of society”;18 Tom Wedgwood’s illness, alas, prevented him from reaching his potential as a scientist.
References
- Wedgwood B, Wedgwood H. The Wedgwood Circle 1730-1897. London: Macmillan Publishing Co.; 1980.
- Litchfield RB. Tom Wedgwood, the First Photographer. Memphis, Tennessee: General Books; 1903.
- Roberts JE, deShazo RD. Abdominal migraine, another cause of abdominal pain in adults. Am J Med. 2012;125(11):1135-9.
- Healey E. Emma Darwin: The Inspirational Wife of a Genius. London: Headline Book Publishing; 2001.
- Azziz R, Woods K, Reyna R, Key T, Knochenhauer E, Yildiz B. The prevalence and features of the polycystic ovary syndrome in an unselected population. The Journal of clinical endocrinology and metabolism. 2004;89:2745-49.
- Wedgwood J. Letter to Thomas Bentley, December 1772. Wedgwood Museum, Barlaston [Internet].
- Pavlakis SG, Phillips PC, DiMauro S, De Vivo DC, Rowland LP. Mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes: a distinctive clinical syndrome. Ann Neurol. 1984;16(4):481-8.
- Mease P, Arnold LM, Bennett R, Boonen A, Buskila D, Carville S, et al. Fibromyalgia syndrome. J Rheumatol. 2007;34(6):1415-25.
- Wallace DC. A mitochondrial bioenergetic etiology of disease. J Clin Invest. 2013;123(4):1405-12.
- Finsterer J. Genetic, pathogenetic, and phenotypic implications of the mitochondrial A3243G tRNALeu(UUR) mutation. Acta Neurol Scand. 2007;116(1):1-14.
- Finsterer J, Zarrouk-Mahjoub S. Frequency of Headache in Mitochondrial Disorders. Headache. 2018;58(2):313-4.
- Fattal O, Link J, Quinn K, Cohen BH, Franco K. Psychiatric comorbidity in 36 adults with mitochondrial cytopathies. CNS Spectr. 2007;12(6):429-38.
- Finsterer J, Strobl W. Brachydactylia as a phenotypic feature of mitochondrial disorder. Acta Med Iran. 2012;50(12):831-5.
- Finsterer J. Pancreatitis as a manifestation of mitochondrial disorder. Am J Med Genet A. 2007;143A(6):632-3.
- Zhang J, Bao Y, Zhou X, Zheng L. Polycystic ovary syndrome and mitochondrial dysfunction. Reprod Biol Endocrinol. 2019;17(1):67.
- Lee WS, Sokol RJ. Mitochondrial hepatopathies: advances in genetics and pathogenesis. Hepatology. 2007;45(6):1555-65.
- Hubble D. Charles Darwin and Psychotherapy. Lancet. 1943;241(6231):129-33.
- Barlow N. The autobiography of Charles Darwin 1809-1882, with original omissions restored. London: Collins; 1958.
JOHN HAYMAN, MD, PhD, FRCPA, is an elderly pathologist still teaching part-time at the University of Melbourne. His interest in the nature of Charles Darwin’s lifetime illness led him to consider the various illnesses that afflicted Darwin’s maternal (Wedgwood) forebears.
Acknowledgment: I am grateful to Lucy Lead, archivist at the Wedgwood Museum, Barlaston, England for Figures 2 and 3 and for corrections to the original manuscript.
Highlighted in Frontispiece Volume 12, Issue 1 – Winter 2020