
JMS Pearce
East Yorks, England
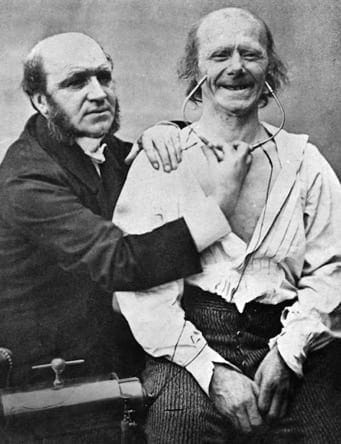
[From Mècanisme de la physionomie Humaine (1862)]
The eponymous Duchenne muscular dystrophy still provokes a sense of sadness in afflicted families and therapeutic impotence in their medical attendants. Although both Edward Meryon (1852) and Wilhelm Griesinger (1865) published early case reports, when Duchenne described the progressive, sex-linked, recessive muscular dystrophy of early childhood, the disorder was almost unknown and its place in the classification of muscle disease uncertain.1,2
Duchenne studied a nine-year-old boy who could not walk because of muscle weakness.3 He gave the details to François Aran, physician to the Hôpital Saint Antoine, who published the case saying: “I owe a thousand thanks to my friend Duchenne de Boulogne who freely put at my disposal all his material.”4 Duchenne himself described “pseudo-hypertrophic muscular paralysis or myosclerotic paralysis,”2 (pp.173-191) in the second, 1861 edition of De l’Electrisation localisée.5 The essentials were: “weakness of the lower limbs with considerable enlargement, since the age of 7 years, leading to progressive generalization of paralysis and complete abolition of all movements at 13.5 years; obtuse intelligence; phthisic death, at 15 years old.” His harpoon muscle biopsies established the pathology.
The author of this work was an extraordinary and highly idiosyncratic, idealistic physician, Guillaume Benjamin Amand Duchenne (1806-1875) (Fg 1.), the son of a long line of seafarers in the region of Boulogne sur Mer.6 He was known as Duchenne de Boulogne to distinguish him from another physician — Duchesne de Paris. His father, a sea captain, who had received the Croix de la Légion d’Honneur from Napoleon, tried in vain to persuade him to follow the family seafaring tradition, however, Duchenne’s love of science prevailed.
He was of medium height, thickset, active in movement, slow of speech, and retained a faint provincial accent.2 He studied medicine in the University of Paris under Laennec, Cruveilhier, and Dupuytren, graduating without distinction in 1831. He returned to Boulogne to general practice, but was so grievously affected by his young wife’s death in childbirth that he lived only for his patients and for his scholarship.
Intensely lonely after his wife’s death he returned to Paris in 1842, “working with an ardour that has rarely been equaled.” Always single-minded, without a formal appointment but with permission of local physicians, he daily visited hospital wards across Paris seeking rare cases of nervous diseases. He described himself as a searcher “… riveted to my own wards.” We would now respect him as a lone outsider.
He questioned and examined patients with laborious obsession, and with perseverance he followed their progress in their homes for many years. At times other physicians ridiculed his provincial accent and coarse manners; he scorned them as “the monarchs of the wards.” Raymond Adams declared that more than any other person of his day he was responsible for developing the technique of meticulous neurological examination.6 His reputation slowly increased, despite a neglect of pathological anatomy and neurological writings. Later in life he concentrated more on the nervous system than on muscles, and turned to histopathology.

Fig 2. Selection from the clinical works of Dr. Duchenne, GV Poore, 1883. [image from personal copy]
Duchenne started to experiment with Faradic current on skeletal muscles, at first seeking treatment for various paralyses, but then investigated electro-muscular contractility as a means to expanding knowledge of their anatomy and physiology. He showed movements were the result of combinations of coordinated activity of associated agonist and antagonist muscles.7
Using this method, in 1852 he began to study facial expression. He believed the face might reveal the inner workings of the mind; it was best recorded by photography, which could render the “truth” of his electrical experiments more effectively than drawings or paintings.8 Of several volunteers his favorite was an old shoemaker seen in many of his well-publicized images. Duchenne published Mécanisme de la physionomie humaine ou analyse électro-physiologique de l’expression des passions (1862) and Physiologie des mouvements (1867). Charles Darwin praised him in his book The Expression of the Emotions in Man and Animals (1872), which contained illustrations based on Duchenne’s photographs.
Eventually Duchenne’s achievements were recognized, among others by the great Jean-Martin Charcot (1825-1893) at the Hôtel de Salpêtrière. Many of Charcot’s scientific approaches were influenced by him, and the young Charcot dubbed him his “mentor” and “the master.” Charcot’s lectures contain frequent acknowledgement of Duchenne’s work. Trousseau also admired him and fostered his recognition.
Neither succinct as a writer nor systematic in his work, his lengthy papers emerged slowly. His first, L’Electrisation Localisée et de son application à la pathologie et à la thérapeutique, was published in 1855 and was well received, encouraging his further research and trials of electrotherapy; by 1872 it had achieved a third edition.
His extensive search for neurological disease and his painstaking, minute analyses led to other important contributions and new descriptions, aided by his use of photography, electrophysiology, and microscopy. He provided original observations of tabetic locomotor ataxia, which contemporaries had confused with Friedreich’s disease, the anterior horn cell lesions of poliomyelitis, glossolabio-laryngeal paralysis (bulbar palsy), and lead palsy. GV Poore collected an invaluable selection of clinical works of Duchenne. (Fig 2.)
In 1862 his previously estranged son Emile joined him in Paris. By this time he had at last gained an international reputation. This culminated in election to many medical societies throughout Europe. A final family disaster occurred when Emile died of typhoid fever in 1871, leaving grave and lasting effects on Duchenne’s life. He died of a cerebral hemorrhage in 1875 with Charcot at his side during his final days.7
His epitaph we can leave to Charcot, who said:
How is it that one fine morning Duchenne discovered a disease that probably existed in the time of Hippocrates? Why do we realise things so late, so poorly, with such difficulty… Because our minds have to take in something that upsets our original set of ideas…
A bas-relief in the Salpêtrière shows Duchenne attending a patient, applying electrodes attached to a simple generator. A modest plaque to a modest man reads:
Duchenne (de Boulogne)
Electrisation Localisée
Physiologie des Mouvements
Neuropathologie
References
- Pearce GW, Pearce JMS, Walton JN. The Duchenne type muscular dystrophy: histopathological studies of the carrier state. Brain, 1966;89 (1):109–120,
- Duchenne GBA. Selections from the clinical works of Dr. Duchenne (de Boulogne). Translated, edited and condensed by G.V. Poore. London, Sydenham Society, 1883.
- Hudgson P. Duchenne’s Dystrophy. In: Koehler PJ, Bruyn GW, Pearce JMS. Neurological Eponyms. New York, Oxford University Press. 2000. Pp. 301-309.
- Aran FA. Archives Génerales de Médicine 1850; 4(sér 24):4–35.
- Duchenne GBA: De l’electrisation localisée. Paris, Baillière 1868; pp. 595–616.
- Adams RD. In: Haymaker W and Schiller F, Eds. The Founders of Neurology. 2nd edn. Springfield. Charles C Thomas 1970. pp.430-434.
- Claraca F, Massion J, Smith AM. Duchenne, Charcot and Babinski, three neurologists of La Salpetrière Hospital,and their contribution to concepts of the central organizationof motor synergy. J Physiol Paris. 2009;103(6):361-76.
- Parent A1. Duchenne De Boulogne: a pioneer in neurology and medical photography. Can J Neurol Sci. 2005;32(3):369-77.
JMS PEARCE, MD, FRCP, is an emeritus consultant neurologist in the Department of Neurology at the Hull Royal Infirmary, England.