
Cynthia Avila
Chicago, Illinois, United States
Sorry indeed should I be, to sport with the life of a fellow-creature who might repose a confidence either in my surgical knowledge or in my humanity; and I should be equally disposed to consider myself culpable, if I did not make every possible effort to save a person whose death was rendered inevitable, if a disease were suffered to continue which it was possible for surgery to relieve.
In the performance of our duty one feeling should direct us; the case we should consider as our own and we should ask ourselves, whether, placed under similar circumstances, we should submit to the pain and danger we are about to inflict.
—Astley Paston Cooper and Benjamin Travers, Surgical Essays, Part 1 (1818), 111–1121
Far beneath the inpatient wards, a scrubbed ensemble of nurses, technicians, physician assistants, and anesthesiologists prepare for a drama that unfolds on the surgeon’s stage. It is here amongst a ceaseless motion that our patient lies, ready to be probed with tools which serve as essential props to the physician’s care. Unconscious, she is privy to the unnatural; a stark absence of relativity radiating beneath the incandescent lights. Surely this is bound to be a good story, because as we all know (and often wish to forget), nothing in the operating room – including the patient’s life – is certain.
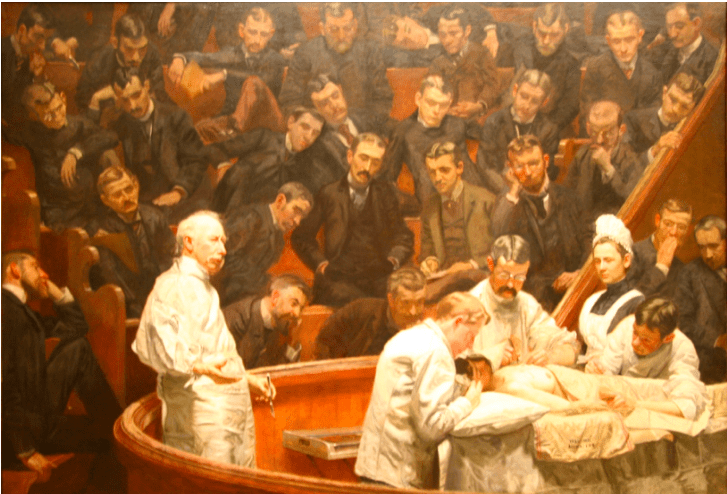
Perhaps as a result of this inherent drama, it is not surprising that operating rooms were once called operating theaters (Wangensteen 1975). Until the 1900’s this nomenclature held true, originating from the wonder that is inseparable from surgery; that is, the fundamental curiousness in dissecting a living human being. It is this curiousness that makes surgery a dramatic enterprise – for although there exists a possibility that the patient will live, so too exists the very real possibility that the patient will die. The patient’s life therefore depends on the surgeon, who acts as the protagonist – the potential hero or executioner, a “tour de force” – in our story. In his account of a surgical procedure in the early 1900’s, Dr. Fredrick Treves (1853–1923) describes his perception of a surgical proceeding as follows: “[the surgeon] stepped into the arena of the operating theater as a matador strides into the ring. Around him was a gaping audience and before him a victim, quivering, terror stricken, and palsied with expectation” (Alpert 2014).2 It is here within the walls of an operating theater that the spotlight shines on the surgeon and the spectacle inherent to his work.
Early characterization of the operation as theatrical reflected an amphitheatric space in which institutionalized surgery originated. In Europe and the United States, several renditions of the operating theater were built to include seating for more than fifty viewers, allowing audience members to observe, smell, and hear the surgeon (and patient) in real time. This seating area was elevated incrementally and permitted spectators a view of the patient, medical team, and tools placed on the instruments table. The audience included colleagues, faculty, medical students and, in earlier presentations, even the general public. This assortment of attendees may seem surprising at first, but what occurred within the operating theater could no doubt provide scholarship and an unrivaled, mysterious form of entertainment for all (Wangensteen 1975).
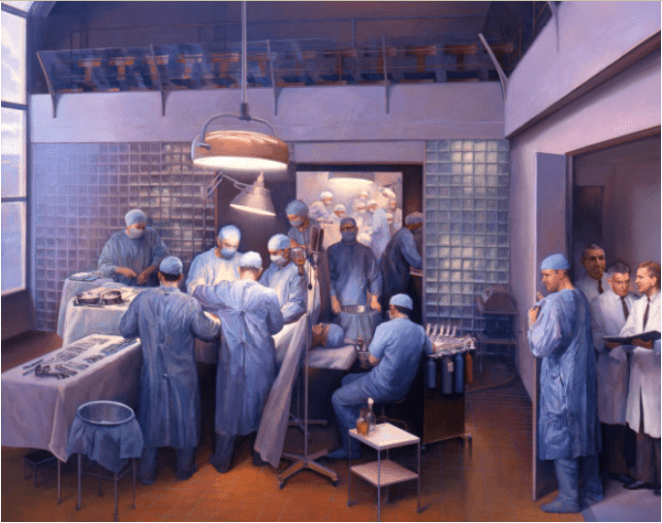
Despite popular attendance at these performances, spectatorship dramatically decreased with the discovery of germ theory and acceptance that public surgeries contributed to post-operative infection (Tait 1887). As a result, operating theaters were remodeled to become an exclusive and sterile space distinctive of operating rooms. In parallel with this transformation, the surgeon’s work became a more calculated and evidence-based practice, where clinical decision-making justified by research was revered. According to Rebecca Barry, author of Inside the Operating Theater: Early Surgery as Spectacle, “by 1917 old-fashioned operating theaters had become obsolete … surgeons began to realize that speed was the variable … causing disastrous results – that indeed slower, meticulous incisions proved more efficacious – there was altogether less drama associated with the surgical stage” (Barry 2014).
By the late nineteenth century, eradication of functional operating theaters would have been complete if not for strong historical preservation efforts. The most famous theaters that remain are the Ether Dome, located at the Massachusetts General Hospital in Boston, and the Old Operating Theater in London. These two historical landmarks were once functional spaces where, as Dr. Treves describes, the surgeon would “step into the arena.” Thousands of operations, predating anesthetics and antiseptics, were performed (Ether Dome, n.d.). Today these amphitheaters remind us of great advancements made in surgical research, training, patient care, and the many unwavering similarities that exist between the surgical and theatric disciplines (The Old Operating Theater & Herb Garret, n.d.).
Understanding the modern-day operating room as former operating theater is essential because it gives meaning to surgical theatrics, a term used to describe governances or routinized acts founded in the art of performance and yet inherent to the surgeon’s work. Examples of surgical theatrics include roles within the medical hierarchy, props to assist the medical team in choreographed procedure, use of apprenticeship in surgical education, and the necessity of an audience to uphold the surgeon’s accountability. These associations produce the following questions: can theatrics be applied to other medical fields and, are theatrics inherent to surgical practice?
The evolution of spectacle
The practice of medicine is an endeavor that is fundamentally emotional, exciting, and therefore dramatic. But theatrics are amplified on the surgeon’s stage more intensely than any other medical discipline as a result of extreme tragedy and triumph, caused by intentional and traumatic human intervention. High stakes, high risk, high stress, procedural degree of uncertainty, disease unpredictability – these are just a few of many factors that contribute to similarities between operating theaters of the past and the operating rooms of the present.
The art of surgery has evolved with biomedical, technological, and pharmaceutical research, but these advancements have not altered the theatrics inherent to a surgeon’s work. As a fundamentally dramatic enterprise, surgical practice continues to display theatrical components which originated from operating theaters of the past. These components are inherent to surgery, even though the spectacle – that is, the visuals and site of production – continue to change. Examples of these surgical components include:
- props (from handheld tools to robotic devices);
- distinct roles (characteristic of the medical hierarchy);
- apprenticeship (as a means of guided and incremental learning); and
- an audience (within the operating room or virtually).
Despite the many analogous features that link surgery with theater, the historiography of surgical theatrics has remained largely untouched. Yet these features are important to explore, not because they bridge medicine with the humanities, but rather because understanding surgical theatrics has the potential to improve surgical training, performance, patient care, and outcomes, as well as the surgeon-trainee and surgeon-patient dynamic. Analysis of surgical theatrics can also open discourse to a range of ethical and philosophical topics, including the surgeon’s moral authority over a vulnerable patient (that is, the ability to make decisions which are right and good) (Brown 2017). Furthermore, these conversations can further address how presentation of emotion – such as fear, compassion, and grief – interplay in the patient and provider experience within the operating room. Although the evolution of spectacle on the surgeon’s stage represents a change in the physical space that operations are held – from operating theater to operating room – the governances and entertainment associated with the surgical art have largely remained consistent over time.
Footnotes
- Brown 2017
- See Frederick Treves, ‘Address in Surgery: The Surgeon in the Nineteenth Century’, The Lancet 156, vol. 2 (1900): 312-317.
References
- The Francis A. Countway Library of Medicine. “Art and Artifacts.” Accessed on February 18, 2018. https://www.countway.harvard.edu/chom/scope-collections
- Alpert, Jessica. “The Art of Surgery: Painting The Operating Room on Canvas.” Accessed on February 18, 2018. http://www.wbur.org/commonhealth/2014/12/17/the-art-of-surgery-painting-the-operating-room-on-canvas
- Barry, Rebecca Rego. “Inside the Operating Theater: Early Surgery As Spectacle.” Accessed February 18, 2018. https://daily.jstor.org/inside-the-operating-theater-surgery-as-spectacle/
- Bosk, Charles. Forgive and Remember: Managing Medical Failure. Chicago: University of Chicago Press.
- Bourdieu, Pierre. Outline of a theory of practice. Cambridge, UK: Cambridge University Press.
- Brown, Michael. “Surgery and Emotion: The Era Before Anesthesia.” The Palgrave Handbook of the History of Surgery. London: Palgrave Macmillian.
- Cassell, Joan. Expected miracles: Surgeons at work. Philadelphia: Temple University Press.
- Davis, Audrey. “The Development of Anesthesia: Techniques of controlling pain transformed the practice of nineteenth-century medicine, particularly surgery and dentistry.” American Scientist, vol. 70, no. 5: 522 – 528.
- Fox, Reneé Claire. Training for Uncertainty. The study-physician: Introductory studies in the sociology of medical education, edited by R.K. Mertn, G.G. Reader, and P.L. Kendall, 207-41. Cambridge, MA: Harvard University Press.
- Hoffman, Stephen. Under the Ether Dome: A Physician’s Apprenticeship at Massachusetts General Hospital. New York: Scribner.
- Holland, J.G. “The Society of American Artists.” Scribner’s Monthly, no. 18: 311-12. http://bit.ly/2EArdGz
- Hunt, Andrew. “American Medicine: The Quest for Competence.” JAMA 275, no. 7 (February): 568-569. https:10.1001/jama.1996.03530310074043
- Lynda Payne. 2007. With Words and Knives: Learning Medical Dispassion in Early Modern England. Ashgate Publishing.
- Morgeli, Christoph. 1999. The Surgeon’s Stage: A History of the Operating Room. Basil: Editiones Roche.
- Newton, Michael. “Moral dilemmas in surgical training: intent and the case for ethical ambiguity.” Journal of Medical Ethics, no. 12: 207-209.
- “Old Operating Theatre Museum & Herb Garret” Accessed on February 18, 2018. https://www.atlasobscura.com/places/old-operating-theatre
- Panda, S.C. “Medicine: Science or Art?” Mens Sana Monograph, vol 4, no 1: 127-139. https://doi10.4103/0973-1229.27610
- Pernick, Martin. A Calculus of Suffering: Pain, Professionalism and Anaesthesia in Nineteenth-Century America. New York: Columbia University Press.
- Polavarapu, Harsha, Kulaylat, Afif, Sun, Susie, Hamed, Osama. “100 years of surgical education: The past, present, and future.” American College of Surgeons: The Bulletin. http://bulletin.facs.org/2013/07/100-years-of-surgical-education/
- Prentice, Rachel. 2007. “Drilling Surgeons: The Social Lessons of Embodied Surgical Learning.” Science, Technology and Human Values32: 535.
- Schatzki, Stefan. “The First Kidney Transplantation.” American Journal of Roentgenology, vol 181, no. 1: (July) 190.
- Schilich, Thomas. “’The Days of Brilliancy are Past’: Skills, Styles, and the Changing Rules of Surgical Performance, ca. 1820-1920.” Medical History, vol 59, no. 3 (July): 379-403. https:10.1017/mdh.2015.26
- Stanley, Peter. 2003 “For Fear of Pain: British Surgery, 1790–1850” Clio Med, vol 70, no. 3: 362.
- Tait, Lawson. “An Address on the Development of Surgery and the Germ Theory.” The British Medical Journal, Vol. 2, No. 1386: 166 – 170.
- Toouli, J. 2006. “What is the role of ‘Live Surgical Demonstrations” at conferences?” HPB, no 8: 163 – 164.
- “The Ether Dome.” Accessed on February 18, 2018. https://www.atlasobscura.com/places/ether-dome
- The Lancet, 3:54 (9 October 1824): 23.
- Wangensteen, Owen, SD, Wangensteen. 1975. “The Surgical Amphitheatre, history of its origins, functions, and fate.” Surgery, vol 77, no. 3: 403 – 18.
- Werbel, Amy Beth. Thomas Eakins: Art Medicine, and Sexuality in Nineteenth-century Philadelphia. New Haven: Yale University Press.
CYNTHIA J. AVILA is a graduate from the University of Chicago with a degree in the History, Philosophy, and Social Studies of Science and Medicine. She is a recent recipient of the Abraham Lincoln Civic Engagement Laureate Award and is the youngest recipient of the 2017 Advocate Illinois Masonic Hispanocare Award. Ms. Avila is currently enrolled in the Health Careers Program at Harvard University and is a Visiting Scholar in Ethics and Medicine at the Hyde Park Institute.
Highlighted in Frontispiece Volume 11, Issue 2– Spring 2019
Leave a Reply