
F. Gonzalez-Crussi
Chicago, Illinois, USA



Those of us who have managed to survive sixty, seventy, or more years remember that the enema or clyster was, by far, the commonest home remedy in the twentieth century. (Enema: “Liquid or gaseous substance, either medicinal or alimentary, introduced mechanically into the rectum.”) No family was without the rubber bottle, the flexible tubing, and the rectal cannula, always ready to assist in the battle against an assortment of ills—as a kind of rearguard reinforcement, if I may be allowed the expression. Sometimes it was not a weapon deployed in combat, but a prophylactic administered to those in blooming health. Italian mothers repeated a proverb: Dieta e serviziale guarisce ogni male (“Diet and enema cure all the ills”). Other cultures extolled the enema’s preventive virtues, and regularly foisted it on defenseless children.
This is remarkable, considering the hoary antiquity of the remedy. According to a tradition, some ancient Egyptians saw the ibis (stork-like bird) preening its plumage with its long beak and concluded that the fowl was giving itself a seawater enema using its beak as a cannula. Why they deemed this a wonderful idea worthy of emulation is beyond me. The oriental mind works in inscrutable ways. But Herodotus (in The Histories, book II, 75-77) and Diodorus Siculus (in his Library of History, book I, 81) assure us that the Egyptians gave themselves enemas monthly.

After these odd beginnings, the practice became universal. Men, lacking a beak, tried to find ways to imitate the ibis. Primitive tribesmen used an animal bladder full of liquid medicament, connected to an improvised tube that was introduced into the patient’s rectum. Manual compression of the bladder impelled the liquid to its destination. Alternatively, they resorted to a hollow dried gourd-shaped somewhat like a maraca. The spheroidal end was the repository of the medicament; the narrowed opposite end went into the patient’s rectum. Blowing into the wide end, through a hole made in it, impelled the medicament. But there was still a simpler method to administer an enema. Loving mothers would lay their babies face down on their lap, apply their lips directly to the anal region of the baby, and blow forcibly the medicament into the baby’s rectum (Fig. 1). Here was a simple and inexpensive method: the impelling force came from the mother’s lungs, with no need for intermediary tools. I gather the need to watch for backflow was its main drawback.
A landmark in the history of the enema was the invention of the syringe. No one knows with certainty who was the inventor. Was it the sages of Alexandria? or the great Arab physicians of the Middle Ages, in particular Avicenna? Or, as scholars contend, a 15th century Italian physician named Marco Gattinara, who was a follower of Avicenna? The fact is, syringes predating the 15th century have been authenticated, but the true origin of this instrument remains enshrouded in the mist of time.
So popular and widespread became the enema that by the 17th century the syringe became the emblem of the health profession, like the caduceus is today. Molière (1622-1673), immortal playwright, pointedly satirized the medicos of his time. In facetious plays, such as “Monsieur de Pourceaugnac” and “The Imaginary Invalid,” the chief protagonist is chased all over the stage by a physician or an apothecary who wields an enormous clyster syringe, while the public doubles up with laughter. At the Louvre Museum there is a painting by an anonymous artist that shows an apothecary holding just such an instrument. It is a forbidding sight (Fig. 2). Most assuredly, if I saw a physician coming at me brandishing this contraption, I would leap out of my bed of suffering, great prostration notwithstanding, and run to the nearest exit.
King Louis XIV, the protector of Molière, had a team of physicians who, perhaps unwittingly, rendered a great service to historians. They kept a meticulous daily record of observations concerning the king’s health, Le Journal de la Santé du Roi. His food, habits, complaints, the appearance of his excretions and dejections: all is carefully noted. If His Majesty so much as sneezed, they wrote it down. Thanks to this compulsive record-keeping we know that Louis XIV received about 2,000 enemas: sometimes up to three a day, during the time that the record was kept. This did not include the last five years of his reign, when his health deteriorated badly. Had the notebook been maintained uninterruptedly, no doubt the number would have been much higher.
Courtiers slavishly imitated the monarch. Louis XIV had an anal fistula and was operated on by his surgeon, Felix. After this, many courtiers boasted of having a fistula without having one. At least thirty applied to the surgeon to have the operation performed on them, and were vexed when they were told that it was not necessary. Similarly, the enema became a fad in the Versailles court. Exalted aristocrats had their own personal syringes; Madame Pompadour owned one in ivory; Cardinal Richelieu had one in silver. Saint-Simon, the court’s renowned chronicler, recounts this anecdote:
The Duchess of Bourgogne chats with Louis XIV behind a balustrade in her apartment. The king notices something unusual in her department and in her companions, but cannot tell what it is. He questions the lady, she is reticent. He insists, and she answers:
“If you really want to know, Sire, I am getting an enema . . .”
“Here?” retorts the king surprised, “Now?” “How can that be possible?”
This bewildered remark elicits some giggles in those present. Immediately, a maid who had crawled under the Duchess’ skirt emerges from behind, letting the posterior part of the skirt fall down, and discretely takes away the enema paraphernalia.
Pre-revolutionary France had the uncanny virtue of eroticizing many aspects of everyday life. The enema did not escape this tendency. The administration of an enema often figures in the art of the ancien régime. But instead of a neutral medical ambiance, the procedure takes place in a boudoir, and the patient is a seductive woman who exposes her private parts to receive the enema while adopting a provocative pose. And, as if to leave no doubt of the libertine nature of the scene, a racy detail may be added: a man furtively peeking through a window, or arriving unexpectedly. The titles of these images are equally suggestive: “The Gentleman Cannot Come in,” “The Ladies’ Pleasure,” and so on (Fig. 3).
A marked advance was due to a brilliant Dutchman, Regnier de Graaf (1641-1672). He connected a cannula to the tip of a flexible tube made of rubber. This eliminated the danger of a rigid syringe’s tip, plus allowing the patient to self-administer the enema. He authored a treatise devoted to the enema, titled De Clysteribus (“On the Clyster”) published in 1668 (Fig. 4). In the 19th century, a French translation appeared with the playful title of “The Instrument of Molière.” I was lucky to have found a first-edition copy in Paris, in a bouquiniste stand, on the banks of the Seine.

De Graaf was one of the most outstanding medical scientists of his time. He wrote important studies on pancreatic and gastric physiology and on genital anatomy. His name has remained in the ovarian “Graafian follicles.” That he should have devoted a whole treatise to the enema demonstrates the historical importance of this therapeutic measure. In his treatise, De Graaf discusses the many classes of enemas, their respective clinical indications, and the recommended techniques of application. Enemas could be, among others: emollient, purgative, astringent, anodyne, detersive, divisive, and even “nutritive.” The latter could contain egg yolk, chicken broth, beef broth, olive oil, red wine, and various other foodstuffs.
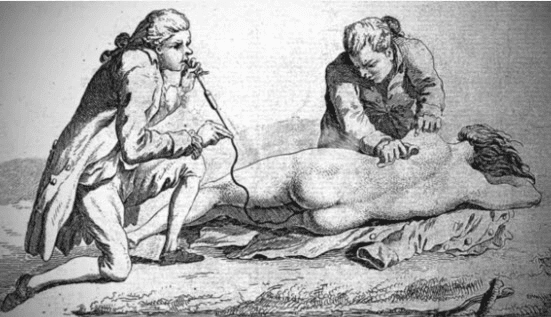
De Graaf did not attempt a comprehensive classification. He makes only a passing mention of the smoke enema. For it is a fact that, based on principles of “humoral” medicine, English physicians came up with the idea of introducing smoke in the intestine of persons who had suffered asphyxia episodes, as in drowning (Fig. 5). Sailors, by virtue of their occupation, were more likely to be involved in drowning accidents. Therefore, in the 18th century, surgeons of the English Navy carried on board their ships the necessary instrumentation to administer this kind of enema (Fig 6). The French translator of De Clysteribus, could not resist making the following quip in a footnote: “What a boon for smokers! Now they can get satisfaction from both ends.” One wonders if tobacco addition explains the fact that smoke enemas were still used as late as 1878, when the French translation of De Graaf’s book appeared.
The age of clysteromania is now past. But modern medicine does not disdain this ancient therapy. Topical administration of corticosteroids, laxatives, preparation for intestinal radioscopic or endoscopic studies, and fecal microbiota transplant are only some of the procedures for which today’s “mainstream” medicine sanctions the rectal route.
Images
- Primitive method of administering an enema, by blowing directly without the use of an injector. From Jacques Frexinos: L’Art de Purger. Paris, Editions Louis Pariente, 1997, p.89.
- Anonymous: Apothecary holding an enema syringe. Louvre Museum, Paris.
- “The Enema,” 18th century French lithograph.
- Fontispice of Regnier de Graaf’s De Clysteribus, Leiden, Officina Hackiana, 1668.
- Administration of a smoke enema to a drowned patient. From A Treatise on Lesser Surgery, or, the minor surgical operations by D.M.P. Bourgery, 1833.
- English naval surgeons’ tool kit to resuscitate drowned patients. Shown are the bellows to propel the smoke, a small chamber to burn tobacco, and the tubing to administer the enema. From Wellcome Images.
F. GONZALEZ-CRUSSI was Head of Laboratories at the former Children’s Memorial Hospital of Chicago (now renamed Lurie’s Hospital) until his retirement in 2001. Born and raised in Mexico, he has authored 20 books of essays, in two languages (English or Spanish). His latest book in English, Carrying the Heart (Kaplan, 2009) won the 2014 Merck Literary Prize in Rome, Italy, for combining medicine and the humanities.