
Jiero Viray
Aberdeen, Scotland

Sleep is a physiological necessity for human life. Humans cycle through two phases of sleep known as rapid eye movement (REM) and non-rapid eye movement (NREM).1 Each stage is associated with varying degrees of muscle tone, brain wave activity, and eye movements. A summary characterizing REM versus NREM sleep is shown in Table 1.
| Table 1: Characteristics of REM versus NREM sleep | ||
|---|---|---|
| Sleep activity | REM sleep | NREM sleep |
| Eye movement | Rapid | Slow (drowsiness) |
| Body movement | Muscle twitches | Muscle relaxation |
| Vital signs | Fluctuating | Stable |
| Muscle tone | Decreased | Some tone in postural muscle |
| Dreams | Common | Rare |
| Electroencephalography (EEG) | Low voltage | Spindles, V-waves, K-complexes, slow waves |
| Percentage (%) occurring in adults | 20–25 | 75–80 |
The term parasomnia originates from the Greek prefix “para” (alongside of) and the Latin word “somnus,” meaning sleep. The term refers to a variety of distressing events that may occur before, during, or after sleep.2 Sleep paralysis (SP) describes a REM-based parasomnia where an individual transitions from REM sleep to a waking state but experiences temporary suppression of voluntary muscle movements. During this transition, individuals are consciously aware of their surroundings. Eye movements and breathing are reported to be less affected.3 Sleep paralysis is often accompanied by hallucinations while entering sleep (hypnagogic) or waking up (hypnopompic), as well as a sense of fear.2
Sleep paralysis affects about 30% of the worldwide population4 and has been well documented throughout history. More recently, SP has been portrayed in popular films and books. Once believed to arise from supernatural causes, research has enhanced our scientific understanding of this sleep condition.5
History
Sleep paralysis has been recognized as the original “nightmare,” as it was historically associated with myths, superstitions, and visitations from evil spirits.3,6 The myth of the incubus, for example, dates back to ancient Mesopotamia (c. 2000 BCE) and translates from Latin as “to sit on,” as in an evil figure sitting on top of one’s chest to induce bad dreams and paralysis.7 A broader use of the term nightmare can be equated with SP and arises from its common usage in historical literature.
Ancient Sumeria (2400 BCE)
In ancient Sumerian folklore, it was believed that the succubus, descendant of the ancient figure Lilith, tormented sleeping victims. Lilith was first described in the Sumerian King List in 2400 BCE, represented as a “she-demon” who would bear the children of men she visited at night to produce demonic offspring.8,9 In the Bible in Isaiah 34:14, she is synonymous with a “screech owl” and the “night monster.” She despised human-born offspring and thus attacked newborns and stripped women of their fertility.9 Some Jewish folklore traditions held that male infants were vulnerable to Lilith prior to covenantal circumcision, though this belief was uncommon.9
Ancient Greece (400 BCE – 216 CE)
The mythical interpretations of nightmares remained as a belief among Greek physicians. Hippocrates is thought to be the first person to describe SP, which the Greeks named “Ephialtes”—“to pounce upon someone.”10 In contrast, Galen did not believe in the supernatural origins of SP and instead speculated that it stemmed from gastric imbalances as a result of overeating or excess alcohol consumption.11
Middle Ages (10th century CE)
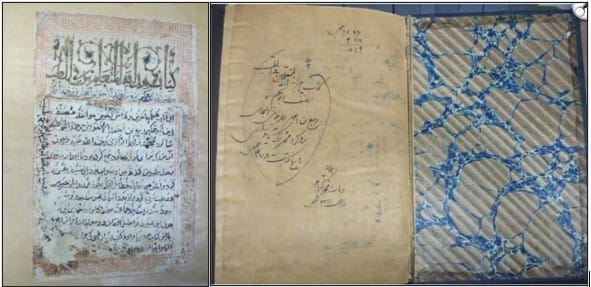
A manuscript named the Hidayat al-Muta’allemin fi al-Tibb reviewed the speculations made by Greek physicians in the form of a medical treatise (Fig 1). It reflected the clinical knowledge gathered from Akhawayni, a Persian physician during the Samanid dynasty (819–999 CE). A chapter of the treatise reveals a section on SP. Like Galen, he speculated on a medical cause—that vapors of phlegm travelled from the stomach to the brain to suffocate sleeping victims. The text also suggests treatments such as purging, venesection, and dietary changes.11 A summary of suggested treatments throughout history is found in Table 2.
| Table 2: A summary of treatment options across different historical periods, taken from various sources | ||
|---|---|---|
| Treatment | Description | Source(s) |
| Ammonia | Drink a solution of ammonia mixed with warm water | Waller, 1816 |
| Astringents | Iron and its derivatives, wild valerian root and a cold bath Pitch plasters | Aurelianus, 1950 Bond, 1753 |
| Bleeding | Therapy includes: bloodletting from the superficial vein in the arm, ankle or leg Bond found that his own practice of 4-6 weeks of bleedings elicited nightmares, so he reduced frequency to once a year Attempt to take pressure of the pulmonary veins and inferior auricle | Aegineta, 1844 Bond, 1753 Golzari et al, 2012 |
| Dietary changes | Thinning of the diet (restrict and attenuate) Avoid difficult to digest/flatulent foods (e.g., cheese, cucumbers, almonds) Add vinegar to meals Eat soft, easy to digest foods Avoid alcohol | Aurelianus, 1950 Bond, 1753 Golzari et al, 2012 Macnish, 1834 Roscher, 2007 Waller, 1817 |
| Evacuants/Purgatives | Induce vomiting/purging using radishes Apply certain ointments to the head (e.g., ones that contain castor) Sneezing and gargling | Aegineta, 1844 Golzari et al, 2012 Macnish, 1834 Roscher, 2007 Waller, 1816 |
| Head shaving | N/A | Aurelianus, 1950 |
| Herbal and vegetable remedies | Black hellebore Hiera (wild gourd) Black pips of peony Scammony mixed with aromatics (e.g., anise, wild carrots, Macedonian parsley) | Aurelianus, 1950 Roscher, 2007 |
| Olive oil | Have patient lie in a moderately lit and warm room and keep mind/body at rest Cover head and region of chest with sourced wool dipped in olive oil Have patient wash mouth with warm water | Aurelianus, 1950 |
| Beaver oil | Rubbed in to help prevent epilepsy | Roscher, 2007 |
| Sleep changes | Not to sleep on their backs (viz., this is the position of dead bodies) Avoid sleeping when slumped over/don’t compress the body (e.g., head resting on a desk while sitting) | Bond, 1753 Macnish, 1834 Van Diemerbroeck, 1689 |
Early Modern Period (17th – 18th century)
In 1664, it could be argued that Dutch physician Isbrand Van Diemerbroeck was the first to describe the symptoms of SP. He produced a collection of clinical case histories from his patients. A specific chapter titled “History XI. Of the Nightmare” translated by William Salmon reveals a case of SP experienced by a fifty-year-old woman.
As cited by Kompanje,12 the following quotations from the chapter can be interpreted:
- “…when she was composing herself to sleep…” Suggestive of SP occurring before sleep onset.“
- …she was not able to stir her members…” Characteristic symptoms associated with SP, such as muscle paralysis and conscious awareness of surroundings.
- “…she believed the devil lay upon her and held her down, sometimes that she was choaked by a great dog or thief lying upon her breast, so that she could hardly speak or breath…” Describes the hallucinatory aspects of SP and belief in a malevolent figure that draws the individual’s efforts to breathe. In many accounts of SP, losing the ability to speak and feeling helpless are reported.6
In 1781, a Swiss artist named Henry Fuseli painted The Nightmare, which, according to Sâ and Mota-Rolim13 represents a classical portrayal of SP. The meaning of the term nightmare has varied over time, and so this painting is said to illustrate the two overlapping meanings. The painting illustrates a sleeping woman, whose nightmare has taken the physical form of an incubus or imp on the chest and a mare, defined as “an evil spirit that torments sleeping humans.”14
20th century
Until the twentieth century, most medical explanations of SP built on Galen’s speculations.10 But Sigmund Freud’s studies of dreams and human behavior introduced new ideas for the origins of SP. Freud proposed that SP stemmed from mental conflict rather than from physiological disturbances.10
Later, Freud’s pupil Ernest Jones published his seminal work on nightmares. He initially proposed that nightmares arose from anxiety because of repressed sexuality. According to Sharpless and Doghramji,2 Jones may have been the first to propose a diagnostic criterion for SP. He proposed several core features of the experience, such as intense feeling of dread, a sensation of pressure or weight on the chest that interferes with breathing, and a conviction of being helplessly paralysed. These characteristics closely resemble what is now recognised as the “incubus” subtype of SP.2
The modern understanding of sleep physiology accelerated after Hans Berger’s development of the EEG in 1929.15 Aserinsky’s study in 1953 was the first documentation of nocturnal eye movements recorded over a whole night. Through EEG readings, he was able to denote the characteristics of REM sleep, which reflected those of a waking state. Subsequent studies would later map the structures and cellular processes associated with REM sleep.
Modern sleep medicine
The pathophysiology of SP is still not fully understood.16 The current understanding is that SP occurs because neurons and transmitters associated with normal REM sleep become dysregulated (Fig 2).16
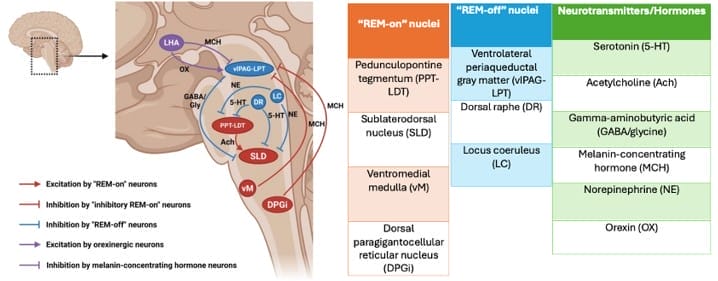
The complexity of neural circuits involved in REM sleep highlight how disruptions in any of these structures lead to commonly reported symptoms in SP. The realization that one cannot move during SP reflects the nightmare experience.9 Furthermore, decreased muscle tone means that breathing may feel labored, which may be interpreted as pressure on the chest. Other types of hallucinations include a threatening presence in the room (intruder) and feeling like one is moving through the air, falling and/or out-of-body experiences (vestibulo-motor).16,18
Narcolepsy
Sleep paralysis may occur independently but is also a core feature of narcolepsy. Narcolepsy is a chronic REM-based sleep disorder characterized by extreme daytime sleepiness, hallucinations, and widespread muscle weakness that can result in collapse.17 After it was observed by Vogel that REM sleep occurred shortly after sleep onset in narcoleptic individuals, researchers concluded that cataplexy and SP reflect the muscle atonia that is attributed to REM sleep.20 Subsequent studies revealed that narcolepsy occurred primarily from a deficiency in the neuropeptide orexin, which is involved in mediating sleep-related symptoms.17,20
Current management of narcolepsy includes non-pharmacological interventions such as improving quality of sleep, addressing mood, and managing underlying mental health conditions.5 Pharmacological interventions, including selective serotonin reuptake inhibitors and tricyclic antidepressants, are also widely used and are speculated to suppress REM properties.3
Conclusion
The original concept of the nightmare is strongly associated with the modern understanding of sleep paralysis. Advances in technology and neurobiology have drawn us closer to its cellular mechanism. Modern sleep medicine has equipped us with the knowledge to treat certain conditions associated with SP symptomatically. Although SP remains poorly understood, in most individuals it is a benign phenomenon.
References
- Patel AK, Reddy V, Shumway KR, Araujo JF. Physiology, Sleep Stages. StatPearls. 2024. https://www.ncbi.nlm.nih.gov/books/NBK526132/
- Sharpless BA, Doghramji K. Sleep Paralysis: Historical, Psychological, and Medical Perspectives. Oxford University Press. 2015.
- Johnson C. Sleep Paralysis: A Brief Overview of the Intersections of Neurophysiology and Culture. American Journal of Psychiatry Residents’ Journal. 2023;18(4). Accessed 24 Nov 2025. https://doi.org/10.1176/appi.ajp-rj.2023.180401
- Honnekeri A. Nightmares or a crippling reality? A review on sleep paralysis. J Family Med Prim Care. 2025;14(7):2639-2642. Accessed 24 Nov 2025. doi:10.4103/jfmpc.jfmpc_212_25
- Sharpless BA. A clinician’s guide to recurrent isolated sleep paralysis. Neuropsychiatr Dis Treat. 2016;12:1761-1767. Accessed 24 Nov 2025. doi:10.2147/NDT.S100307
- Olunu E, Kimo R, Onigbinde EO, Akpanobong M-AU, Enang IE, Osanakpo M et al. Sleep Paralysis, a Medical Condition with a Diverse Cultural Interpretation. International Journal of Applied and Basic Medical Research. 2018;8(3):137-142. Accessed 24 Nov 2025. doi:10.4103/ijabmr.IJABMR_19_18
- Jaffray S. The cures and demons of sleep paralysis. Welcome Collection Stories. 2016. https://wellcomecollection.org/stories/sleep-paralysis-a-brief-history-of-fear-treatment-and-artistic-creativity
- Cox AM. Sleep paralysis and folklore. JRSM Open. 2015;6(7). Accessed 25 Nov 2025. doi:10.1177/2054270415598091
- Adler SR. Sleep Paralysis: Night-Mares, Nocebos, and the Mind-Body Connection. Piscataway: Rutgers University Press; 2011.
- Davies O. The Nightmare Experience, Sleep Paralysis, and Witchcraft Accusations. Folklore. 2003;114(2). Accessed 25 Nov 2025. doi:10.1080/0015587032000104211
- Golzari SEJ, Khodadoust K, Alakbarli F, Ghabili K, Islambulchilar Z, Shoja MM, et al. Sleep paralysis in medieval Persia – the Hidayat of Akhawaynic (?-983 AD). Neuropsychiatr Dis Treat. 2012;8:229-234. Accessed 25 Nov 2025. doi:10.2147/NDT.S28231
- Kompanje EJO. ‘The devil lay upon her and held her down’: Hypnagogic hallucinations and sleep paralysis described by the Dutch physician Isbrand van Diemerbroeck (1609-1674) in 1664. Journal of Sleep Research. 2008;17(4):464-467. Accessed 26 Nov 2025. https://doi.org/10.1111/j.1365-2869.2008.00672.x
- R. de Sá J, Mota-Rolim SA. Sleep Paralysis in Brazilian Folklore and Other Cultures: A Brief Overview. Front. Psychol. 2016;7. Accessed 25 Nov 2025. https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2016.01294/full
- Paulson N. “Henry Fuseli, The Nightmare.” Smarthistory. 2015. Accessed 25 Nov 2025. https://smarthistory.org/henry-fuseli-the-nightmare/
- Lemke J, Kluger G, Krämer G. Hans Berger and 100 years of the electroencephalogram. Clinical Epileptology. 2024;37:112-119. Accessed 26 Nov 2025. https://doi.org/10.1007/s10309-024-00704-6
- Wróbel-Knybel P, Flis M, Dubiel R, Karakula-Juchnowicz H. What do we know about sleep paralysis? Curr Probl Psychiatry. 2018; 19(3). Accessed 27 Nov 2025. doi:10.2478/cpp-2018-0014
- Wang Y, Li Q, Zhong Z, Ouyang Q, Zou X, Yue K et al. Sleep Paralysis: Pathogenesis, Clinical Manifestations, and Treatment Strategies. J. Integr. Neurosci. 2025;24(8). Accessed 27 Nov 2025. doi:10.31083/JIN38979
- Ableidinger S, Holzinger B. Sleep Paralysis and Lucid Dreaming – Between Waking and Dreaming: A Review about Two Extraordinary States. J. Clin. Med. 2023;12(10). Accessed 27 Nov 2025. https://doi.org/10.3390/jcm12103437
- Newsom R. Sleep Paralysis Demon. By SLEEP DOCTOR. 2025. Accessed 27 Nov 2025. https://www.sleepfoundation.org/parasomnias/sleep-demon
- Shepard Jr JW, Buysse DJ, Chesson Jr AL, Dement WC, Goldberg R, Guilleminault C et al. History of the Development of Sleep Medicine in the United States. J Clin Sleep Med. 2005;1(1):61-82. Accessed 27 Nov 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC2413168/#R12
JIERO VIRAY is a third-year medical student at the University of Aberdeen. This article was revised from coursework for a six-week medical humanities block and reflects his interest in the origins of sleep paralysis and its current understanding in clinical medicine.