
Eric Will
Nicholas Marks
United Kingdom
“Tinkering” is a mindset that responds to calls for improvement or repair through piecemeal modification. It may involve novelty or rediscovery, and ranges from mechanics to imaging, the concrete to the abstract. A writer tinkers with a text, the artist with a canvas, the mechanic with an engine. It is generally improvisatory and seeks the progressive perfection of its object, or perhaps a change in the way it is used.
Tinkering occurs all the time in medicine, not least in the trial and error of diagnosis and treatment or research driven by curiosity. It often precedes the consolidation of a new technology and is a process that is behind medical progress of all kinds. However, once proof of principle has been achieved, an introduction to routine practice has always needed careful tailoring. Indeed, a common pattern of difficulty is apparent in post-tinkering implementations, which overtake, in scale, the tinkering dimension.
In the 1950s, the drive to develop hemodialysis was international and stimulated tinkering medical individuals, sometimes regardless of the consequences for their careers or status in the specialty.1-3 Subsequently, the rescue of patients with reversible acute kidney failure became demonstrable in the UK and the dialysis methodology recognized as refined enough for routine use.4 The transfer to formal implementation was the awarding of responsibility for maintenance hemodialysis in the UK to regional health authorities in 1966 and their development of kidney replacement facilities. Of course, technical development continued as commercial resources were gradually brought to bear. The early expansion of treatment piloted through the in-house, piecemeal, proliferation of local (satellite) hemodialysis centers was usurped ultimately by the demanding maintenance of increasingly sophisticated machines and the economies of scale in commercial provision by equipment companies.
Other renal specialty sectors can be considered as passing through a not dissimilar sequence of improvisation recast by an overtaking routine. For example, the progressive computerisation of clinical renal activity, documented in the British Renal Computing Group meetings of 1981–1989, was a kind of tinkering by enthusiasts that demonstrated the extent to which practice could be facilitated and improved.5 That initiative was overtaken by a UK programme of IT (NPfIT), with the intention to computerise the entire National Health Service. The hubris of that ambition cost a great deal of national treasure (£12bn) for little ultimate benefit. The failure to reap what had been sown in widespread renal unit tinkering was manifest!
Then again, the mid-1990s intention to support evidence-based medicine through a UK Renal Registry could not spring fully formed from established theory and practice, but was gradually shaped by trial-and-error approaches to data presentation and evaluation from 1997–2011. Quality assurance was arguably less familiar ground than epidemiology.6
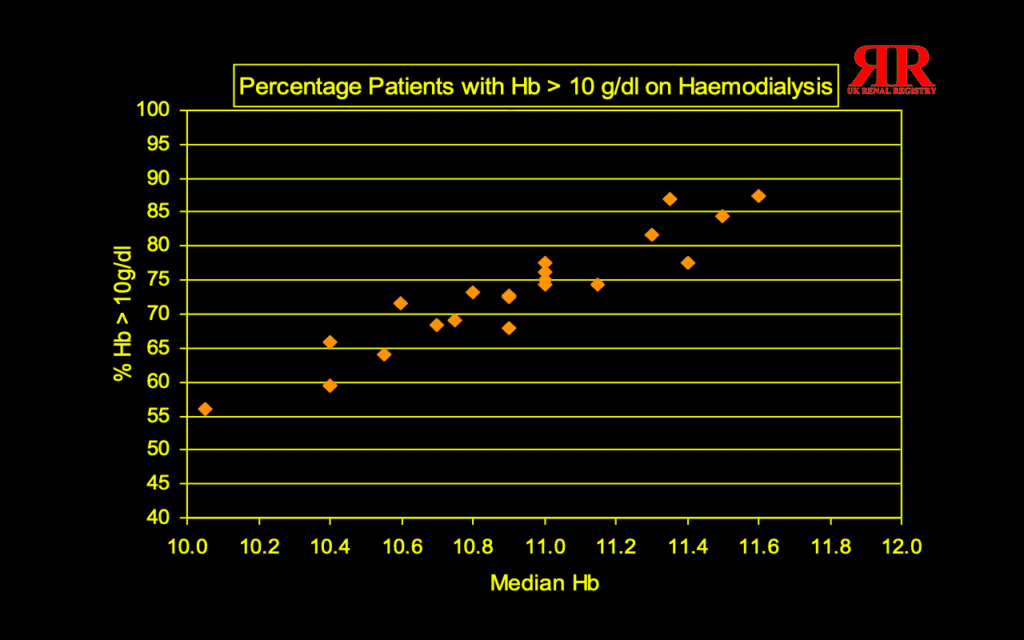
An example of a new approach was the use of adapted Rose-Day plots to indicate renal center goals necessary to achieve the recommended anemia management and dialysis dose. The progressive improvement in unit results was first scoped and then tracked over fourteen years to near complete compliance.7,8 In the event, the transition to routine annual registry reporting was not without significant disruption in personnel and development as tinkering was superseded. The development of AI, as another general facilitatory technology, is likely to offer more opportunities for tinkering in medical practice.
It seems likely that the selection of medical students has always involved implicit testing for the tinkering mindset. It overlaps with enthusiasm and prowess in problem solving. This intuitive dimension is so universal in practice that it has scarcely earned a name or structure. In recent times, it is becoming appreciated as an explicit educational approach in order to encourage inventiveness and self-respect.9 That recognition can be considered an example of a notable discipline emerging from its own, only too provisional, methodology!
References
- Peitzman SJ. Origins and Early Reception of Clinical Dialysis. Am J Nephrol 1997;17 (3-4): 299–303.
- Will E. Frank Parsons—A hemodialysis pioneer. Hektoen Int Winter 2024. https://hekint.org/2024/03/14/frank-parsons-a-hemodialysis-pioneer/
- Rosen SM, Cameron JS. Stanley Shaldon. UK Kidney Association. https://www.ukkidney.org/about-us/history/obituaries/stanley-shaldon
- Turney JH, Blagg CR, Pickstone JV. Early dialysis in Britain: Leeds and Beyond. Am J Kidney Dis 2011;57(3):508-515.
- Will EJ, ed. Perspectives on UK clinical renal computing 1979–1994. Seminar at the Royal College of Physicians, July 19-20, 2017. UK Kidney Association. https://www.ukkidney.org/sites/renal.org/files/history/Clinical-renal-computing-Witness-Seminar.pdf
- Will EJ. Intention and Outcome in Guideline-based nephrological practice: a suitable space for “clinical technology.” Nephrol Dial Transplant 2007; 22:3110-4.
- Rose G, Day D. The population mean predicts the number of deviant individuals. Br Med J 1990; 301:1031-1034.
- Annual Reports. UK Kidney Association. https://www.ukkidney.org/audit-research/annual-report/all
- Mader A, Dertein E. Tinkering as method in academic teaching. International Conference on Engineering and Product Design Education, September 8-9, 2016, Aalborg University. University of Twente. https://www.utwente.nl/en/eemcs/educational-quality/archive/Results/publications/tinkering/made2016-tinkering-as-method-in-academic-teaching.pdf
ERIC JOHN WILL graduated from Oxford University and Guy’s Hospital, followed by research in the Netherlands on renal stone disease from 1977–1979. He was a teaching hospital renal physician from 1980–2007; his personal research has included analysis of clinical intention, medical decision support, and RCTs in renal anemia. His national positions have included chair of the British Renal Computing Group from 1981–1989 and secretary to the UK Renal Registry from 1997–2007.
NICHOLAS JOHN MARKS graduated from London University and Guy’s Hospital and subsequently worked in London and Reading as a head and neck surgeon with a special interest in skin flaps and their physiology. He carried out basic research in this field at the University of Washington, Seattle. Other clinical interests have included endoscopic nasal surgery and facial pain.