
Victoria Tiller
Glenview, Illinois, United States

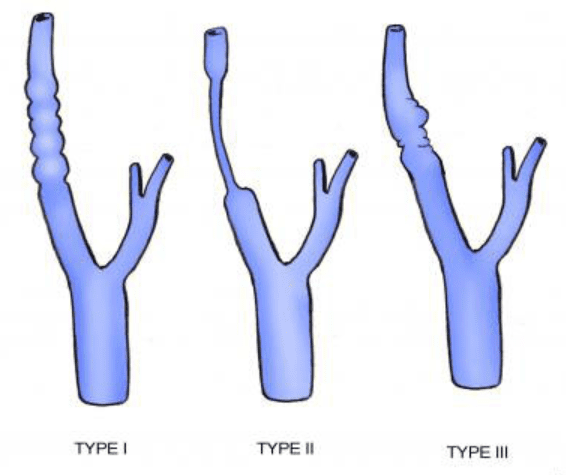
I. String of beads
II. Long central stenosis
III. With diverticular outpouching
Fibromuscular dysplasia (FMD) is a disorder of the arteries, most often affecting the carotid, vertebral, and renal arteries. The interior arterial lining grows abnormally to create intermittent narrowing within the vessel, resulting in “arterial beading” or a “string of beads” on imaging studies. Historically, the condition has often been overlooked or minimized. However, FMD can increase the risk of complications and poor outcomes, especially when there are concurrent conditions such as atherosclerosis. Perhaps in part because it is underdiagnosed, FMD is still considered rare by the National Organization of Rare Diseases (NORD).
Nurses and physicians should consider FMD in the differential diagnosis for patients who present with severe headache, hypertension, transient ischemia attack (TIA), or stroke-like mimics. If the history, physical, and imaging studies are suggestive of FMD, full body arterial imaging should be performed to locate evidence of multi-focal disease. A missed or overlooked diagnosis can lead to devastating outcomes. Those who live with FMD may receive treatment, be followed with surveillance, and be educated about ways to decrease the risk of adverse outcomes.
FMD is still by far, more common in women. Infants, children, and men are being diagnosed in greater numbers. In 2024, emergency alert cards and medic alert bracelets were made available, which outline the approach to a person with FMD in an emergency.1 The emergency alert card offers awareness and diagnostic suggestions when an FMD patient presents with severe abdominal pain, headache, chest pain, or symptoms of stroke should be considered for urgent vascular evaluation. These patients, when appropriate, should raise a concern for arterial dissection or aneurysm.

In the US, nineteen clinics now gather data and are developing strategies to identify and address FMD.2 As of May 2024, there were about 4,400 patients around the world enrolled in the FMD registry, an increase from just 447 enrolled in 2012.3
FMD was first identified by two pathologists around 1938. But without high-resolution imaging to identify more people with the condition, diagnosis and research lost prominence. Today, however, the Texas Heart Institute has labeled FMD as “the rare disease that isn’t,” suggesting that its prevalence is higher than previously believed.
As with any rare disease, awareness is our greatest contribution. Researchers and practitioners now caution patients with FMD in carotid and vertebral arteries to avoid hyperextending the neck, lifting more than 25 pounds, deep neck massage, and chiropractic manipulation. That warning could postpone or avoid damaging fragile arteries susceptible to tearing or dissection. Arteriography and ultrasound, statins, low dose aspirin, anti-hypertensives, genetic evaluation, and inclusion in the FMD registry are all offered as part of the standard protocol. As with any rare disease, greater recognition and improved treatment options begin with the painstaking steps of identifying prevalence.
References
- Fibromuscular Dysplasia Society of America. Medical alert card and bracelet. 2024. Accessed December 2024. https://www.fmdsa.org/wp-content/uploads/2024/05/emergency-card-final-2024-No-Address-1.pdf
- Fibromuscular Dysplasia Society of America. Research Network, North American Registry for FMD. Accessed December 2024. https://www.fmdsa.org/research-network/
- Olin JW et al. “The United States Registry for Fibromuscular Dysplasia: Results in the First 447 Patients.” Circulation 125, no. 25, (2012): 3182-90.