
JMS Pearce
Hull, England
William John Adie (Fig 1) deserves to be remembered as an unusually gifted, compassionate clinician and teacher, but he is best known for his account of the myotonic (Holmes-Adie) pupil.
One of many talented Australians who enhanced British medicine, Adie was born in Geelong, west of Melbourne. He was educated at Flinder’s School, but at the age of thirteen had to leave in order to support the family after his father’s death—a tough and testing beginning. He worked as a humble office errand-boy, but fortunately one of his employers recognized his abilities and paid for his further education. A brief spell of unskilled tasks assisting general practitioner Arthur South of Geelong inspired Adie to embark on a medical career. But medical school fees in Melbourne were high and an uncle paid for his nineteen pounds one-way ticket to England. He obtained a scholarship that enabled him to read medicine at Edinburgh, where he graduated in 1911.
He then ventured to Berlin, Munich, Vienna, and Paris for clinical experience before he was appointed house physician to the National Hospital Queen Square. This was “the golden era of neurology” succeeding Sir William Gowers, which included: Gordon Holmes, Henry Head, FMR Walshe, Kinnier Wilson, CP Symonds, Macdonald Critchley, and Russell Brain.a Despite attempts by his uncle to bring him back to Australia, Adie’s affection for Britain led him to spend the rest of his life there.
At the outbreak of the First World War, he joined the Northamptonshire Regiment and served as medical officer in France, where he took part in the retreat from Mons; his regiment was annihilated. In 1916 he was mentioned in dispatches for saving the lives of soldiers in mustard gas attacks by devising a mask of clothing soaked in urine. He subsequently took charge of the 7th General Hospital and was consultant in the management of head injuries.1
After the war he became medical registrar in the Charing Cross Hospital. He obtained the MRCP in 1919, FRCP in 1926, and the MD Edinburgh with gold medal in the same year. In 1916 he married Lorraine Bonar; they had a daughter and a son. He was appointed to the staff of the National Hospital, Queen’s Square, and Moorfields Eye Hospital.8
His clinical acumen and diagnostic skill were soon evident; “His was the method of rational discourse and discriminating observation, like that of Sherlock Holmes in a white coat.”2 His teaching was brilliant and he displayed great compassion for his patients, quickly perceived by his students.3 With Macdonald Critchley he described in frontal lobe disease: “A syndrome of forced grasping and groping.”4 He lucidly described narcolepsy,5 and wrote important papers on inter alia, pituitary tumors, myasthenia gravis, dystrophia myotonica, familial periodic paralysis, hepato‐lenticular degeneration, and disseminated sclerosis. With his friend James Collier, he wrote the section on neurology in Price’s Textbook of the Practice of Medicine, considered the finest general textbook account of neurology.
He was a founder of The Association of British Neurologists.b Sadly, when aged forty-five Adie developed angina and in 1935 was obliged to resign his post when only forty-eight. He died from a myocardial infarct on March 17, 1935.
Adie was admired for his intelligence and powers of shrewd clinical observation. Above all, he was esteemed as a modest generous man who was loved by his students. In his native town, the boy who had accomplished so much on the other side of the world was not forgotten. The daily newspaper Geelong Advertiser headed an obituary: “Geelong boy who made good in London.”
Adie’s Syndrome
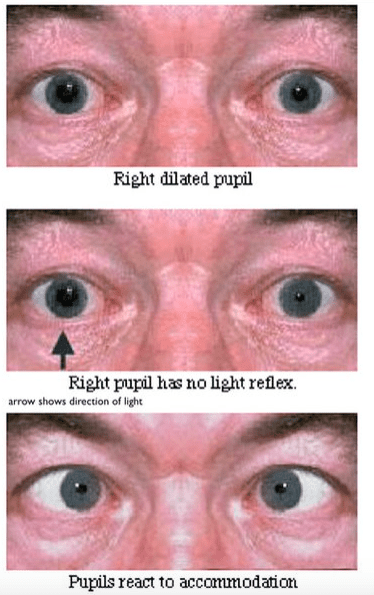
Fig. 2. The myotonic pupil. (Arrow shows direction of light)
From the National Hospital, Queen Square in 1931 he described the harmless condition of a dilated pupil which reacts abnormally slowly (myotonic) to light but reacts normally to accommodation.2,6 (Fig 2)
I wish to draw attention to a benign symptomless disorder characterized by pupils which react on accommodation but not to light, and by absent tendon reflexes. Five of the six cases I am about to describe came under my notice in the course of a few weeks . . . Though harmless in itself it merits recognition because it is often mistaken for a manifestation of syphilis of the nervous system, with unfortunate consequences . . . Mr. Foster Moore has described seven cases under the title ‘Non-luetic Argyll Robertson pupil.6
Commonly known as the Holmes-Adie pupil, the reaction of the pupil is sluggish and is usually unilateral, most often seen in women, commonly with absent leg tendon reflexes. The pathology was localized to the ciliary ganglion by Harriman and Garland,7 who credited earlier papers dating back to 1902 by Strassburger in a seventeen-year-old man, and by Alfred Saenger in the left pupil of a thirty-four-year-old woman.
Adie later described thirteen patients with absent tendon reflexes and noted forty-four reported cases of tonic pupil. It dilated promptly to drops of atropine and constricted with physostigmine8 and methacholyl, which showed parasympathetic denervation hypersensitivity.9 In an exemplary clinical essay,10 Adie outlined a complete form—typical tonic pupil and absence of reflexes —and four incomplete forms (the last would not now be accepted):
Incomplete forms:
a) tonic pupil alone; b) atypical phase of the tonic pupil alone (iridoplegia; internal ophthalmoplegia); c) atypical phases of the tonic pupil with absent reflexes; d) absent reflexes alone.
Gordon Holmes described the same disorder in 1931 but like descriptions before Markus and Adie, Holmes failed to emphasize the areflexia.11 Adie did not claim originality. Hughlings Jackson in 1881 had earlier provided a convincing account,12 and Adie acknowledged papers by the London ophthalmologist James Ware (1756–1815) in 1813,13 and those of Markus,14 Nonne, Strassburger, and Saenger in 1902.
End Notes
- Russell Brain was on the staff of Maida Vale and the London hospitals but not at Queen Square.
- The ABN was initiated at a meeting in the house of Gordon Holmes at 9 Wimpole Street, on July 28th 1932. Present were: W J Adie, E Bramwell, E F Buzzard, H Cohen, J S Collier, D E Core, A Feiling, R G Gordon, J G Greenfield, G Hall, W Harris, W Johnson, F J Nattrass, C Worster-Drought, S A Kinnier Wilson, and G Holmes.
References
- Adie WJ, Wagstaffe WW. A note on a series of 656 cases of gunshot wound of the head, with a statistical consideration of the results obtained. London, H.M. Stationery Off., 1918. Medical Research Committee Statistical reports, no. 1.
- Bruyn GW, Gooddy W. Adie’s syndrome. In: Neurological Eponyms. edited Peter J. Koehler PJ, Bruyn GW, Pearce JMS.Oxford, OUP 2000; Pp. 181-185.
- Pearce JMS. William John Adie (1886-1935). J Neurol Neurosurg Psychiatry. 2004 Aug;75(8):1111.
- Adie WJ, Critchley M. Forced grasping and groping.. Brain, 1927, 50: 142-170.
- Adie WJ. Idiopathic narcolepsy: a disease sui generis: With remarks on the mechanism of sleep. Brain 1926; 49: 275-306.
- Adie WJ. Pseudo-Argyll Robertson pupils with absent tendon reflexes. A benign disorder simulating tabes dorsalis. British Medical Journal, London, 1931;I:928-930.
- Harriman DGF, Garland H. The pathology of Adie’s syndrome. Brain 1968; 91; 401-18.
- Siddiqui AA, Clarke JC, Grzybowski A. William John Adie: the man behind the syndrome. Clin Exp Ophthalmol. 2014;42(8):778-84.
- Scheie HG. Site of disturbance in Adie’s syndrome. Arch Ophthalmol 1940; 24: 225–237.
- Adie WJ. Tonic pupils and absent tendon reflexes: a benign disorder sui generis; its complete and incomplete forms. Brain 1932; 55 : 98-113.
- Holmes G. Partial iridoplegia associated with symptoms of other diseases of the nervous system. Trans Ophthal Soc. UK. 1931; 51 : 209-28.
- Pearce JMS. Hughlings Jackson and the Holmes-Adie tonic pupil. In: Fragments of Neurological History. London, Imperial College Press. 2003. pp. 249-251.
- Ware J. Philos Tr Roy Soc. London 1813; 31-50. [see Dunn’s biography of Ware. Br J Ophth 1917; 1 :401-10.] cited by Leake CD. In: Founders of Neurology. Ed W. Haymaker and F. Schiller. 2nd edn. Springfield, Illinois: Thomas. 1970. pp. 505-6.
- Markus C. Notes on a peculiar pupil-phenomenon in cases of partial iridoplegia. Trans Ophthalmol Soc UK 1906;26:50-58.
JMS PEARCE, MD, FRCP, is an Emeritus Consultant Neurologist Department of Neurology, Hull Royal Infirmary, and an author with a particular interest in the history of science and medicine.