
Charles Kels
San Antonio, Texas, United States
The law of war is enshrined in treaties but steeped in blood.
In 1859, a young Swiss businessman was traveling through Italy when a savage battle between French and Austrian forces commenced. Seeing “how many unfortunate men were left behind, lying helpless on the naked ground in their own blood,” Henry Dunant sought to render aid in the grisly aftermath.1
He observed. He recorded. “With faces black with the flies that swarmed about their wounds, men gazed around them, wild-eyed and helpless. Others were no more than a worm-ridden, inextricable compound of coat and shirt and flesh and blood.” Beloved husbands, sons, and fathers had gone to war; now “all lie stretched in the mud and dust, drenched in their own blood! The handsome manly face is beyond recognition, for sword or shot has done it disfiguring work. The wounded man agonizes, dies and his dear body, blackened, swollen and hideous will soon be thrown just as it is into a half-dug grave.”1
Dunant also proposed action. He advocated relief societies to care for the wounded. And he championed law, promoting an “international principle, sanctioned by a Convention inviolate in character” to enable the relief societies in their healing work. The task was urgent, for “when hostilities once begin,” it is already too late for agreement.1
Dunant’s descriptions and recommendations soon provided the animus for a worldwide movement to ameliorate suffering in war. In 1863, a five-person committee including Dunant and two physicians held the first meeting of what would become the International Committee of the Red Cross (ICRC). The following year, they convened a conference of sixteen nations that produced the first Geneva Convention.2
From the outset, medical care and those who render it were placed front and center in the humanitarian movement.3 The first Convention established that hospitals, ambulances, and the personnel who staff them were to be considered neutral, and thus “protected and respected,” regardless of nationality.2 Under the Geneva framework, medics and chaplains are deemed to “stand above the fighting” so they can minister to individuals’ health and spiritual needs. In turn they must abstain from fighting themselves so as not to jeopardize their own immunity and, more importantly, that of the patients and worshipers they serve.3 Healing and combatancy are incompatible.
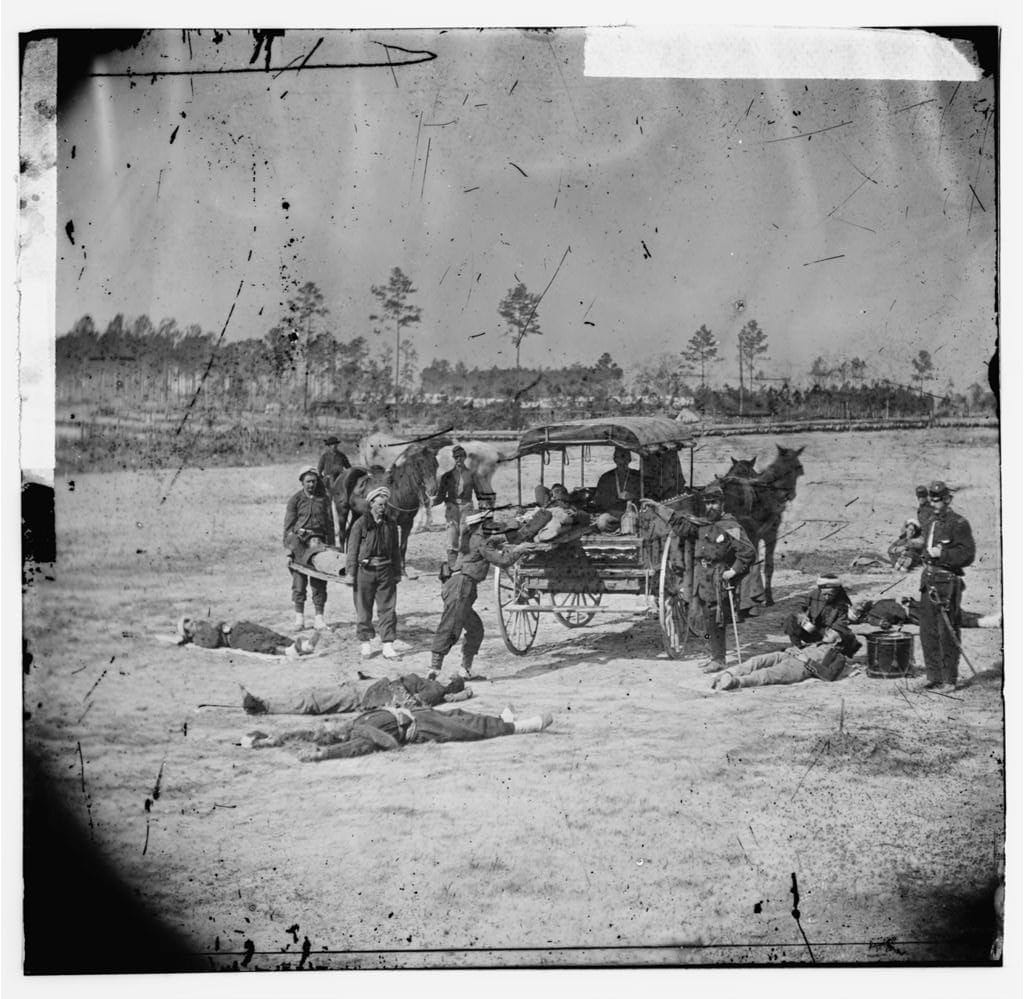
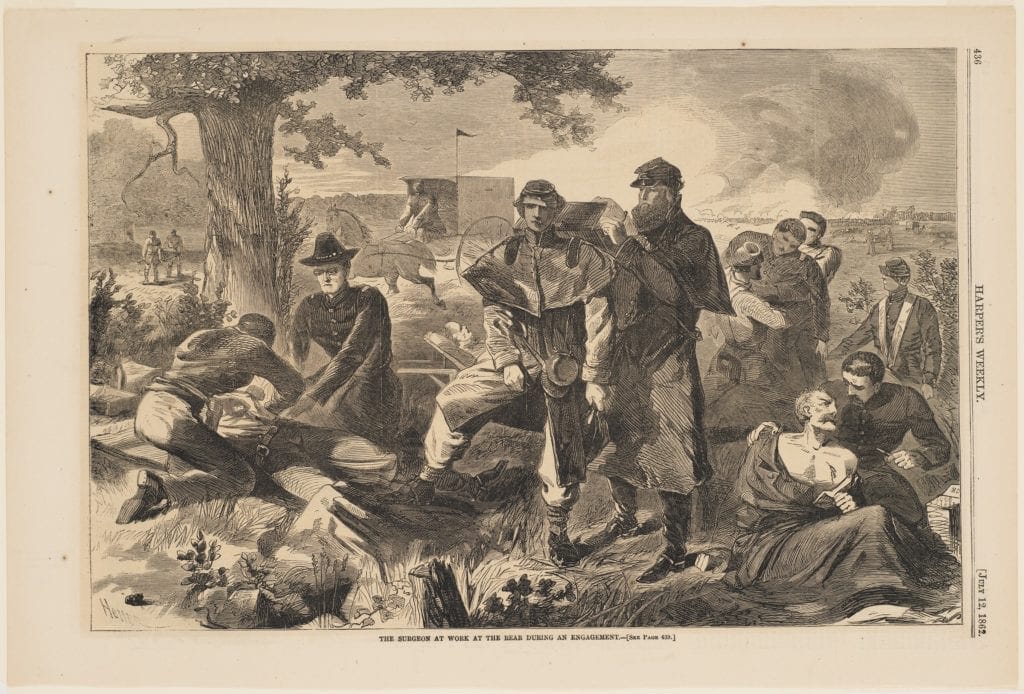
Meantime, across the Atlantic the Americans—embroiled in bloody civil strife—had come to similar conclusions about the primacy of medicine in regulating warfare and mitigating its worst excesses.4 General Orders Number 100, promulgated by President Abraham Lincoln in 1863, instructed the Union army to treat wounded Confederate soldiers upon capture and to release Confederate medical personnel unless their services were needed.5 Lincoln’s general orders are widely considered the first modern codification of the rules governing conduct in war.6 Despite battlefield medicine’s rudimentary state, the sheer carnage and destruction of the U.S. Civil War underscored the need to prioritize it. Whereas the Union surgeon general later remarked that the war was fought at “the end of the medical middle ages,” Enlightenment principles of humanity imbued the efforts to codify its protected status.7
Over time, the legal protections for medical care in wartime have been strengthened and refined.8 It is now firmly established that no person, whether military or civilian, may be “molested or convicted for having nursed the wounded or sick,” irrespective of the patient’s enemy status.9
Perhaps more significantly, medical ethics have been incorporated into international law itself.3 Medical personnel who are captured and retained by the enemy to treat prisoners of war must be permitted to practice “in accordance with their professional ethics.”9 Health care providers may not be compelled to act “contrary to the rules of medical ethics,” nor may they be punished “for carrying out medical activities compatible with medical ethics.”10 Such legal deference to professional norms reaffirms that for those entitled to wear the red cross emblem, the medical role is always paramount.11
Yet the world stands at a crisis point for medical care in armed conflict. Attacks on health care workers and health care facilities have reached epidemic proportions.12 Syria and Yemen have become particularly deadly territory for doctors, with increasing evidence that Syrian government forces have systematically targeted medical workers in flagrant contravention of the most fundamental tenet of humanitarian law.13 In other conflict zones, armed groups have deliberately positioned military assets in and around medical facilities, thereby compromising vital protections for all doctors and patients in the quest for military or public relations gain.14 The precarious situation of health care personnel was exacerbated by the tragic series of errors and failures leading to a deadly U.S. airstrike on a Médecins Sans Frontières hospital in Afghanistan in 2015.15,16
The president of the ICRC has called attention to the vital need to protect health care in the face of violence against its delivery.17 In response to increasing threats, the Red Cross launched a multi-pronged awareness and mobilization campaign,18 and the United Nations Security Council resolved to strengthen the protection of wartime medical care.19
Efforts to bolster humanitarian safeguards in war emphasize their underlying fragility. Just as health care workers seek to mitigate war’s horrors with the power of healing, law aims to erect guardrails on conflict with the power of words.3 Medical care and those who provide it have been at the heart of the rules governing warfare since their very inception. Health care and humanitarian law are inextricably linked.
In the face of rampant disregard for the foundational norms of international law, it is more imperative than ever to return to, and clearly enunciate, first principles. Medical personnel and facilities must never be attacked, and medical insignia and assets must never be misused. If we do not protect the protectors, this central humanitarian compromise animating the law of war is put at dire risk. Over a century and a half later, Dunant is still calling the world to action.
References
- Dunant H. A Memory of Solferino (1862). Geneva: International Committee of the Red Cross; 1986. https://www.icrc.org/en/publication/0361-memory-solferino#. Accessed January 10, 2020.
- Geneva Convention for the Amelioration of the Condition of the Wounded in Armies in the Field. August 22, 1864. https://www.icrc.org/en/doc/resources/documents/treaty/geneva-convention-1864.htm#gs.rybhjn. Accessed January 13, 2020.
- Pictet J. The medical profession and international humanitarian law. Int’l Rev of the Red Cross. 1985;247:191-209.
- Bosco D. Moral principle vs military necessity. Am Scholar. Winter 2008. https://theamericanscholar.org/moral-principle-vs-military-necessity/#.Xh6Gtm5Fw2w. Accessed January 14, 2020.
- Lincoln A. General Orders No 100, Instructions for the Government of Armies of the United States in the Field. April 24, 1863. https://avalon.law.yale.edu/19th_century/lieber.asp. Accessed January 14, 2020.
- Baxter RR. The first modern codification of the law of war: Francis Lieber and General Orders No 100. Int’l Rev of the Red Cross. 1963;25:171-189. https://www.loc.gov/rr/frd/Military_Law/pdf/RC_Apr-1963.pdf
- Faust DG. This Republic of Suffering: Death and the American Civil War. New York: Vintage; 2008.
- Lewis DA, Modirzadeh NK, Blum G. Medical care in armed conflict: international humanitarian law and state responses to terrorism. Harvard Law School Program on International Law and Armed Conflict. September 2015. https://pilac.law.harvard.edu/medical-care-in-armed-conflict-international-humanitarian-law-and-state-responses-to-terrorism. Accessed January 12, 2020.
- Geneva Convention I for the Amelioration of the Condition of the Wounded and Sick in Armed Forces in the Field. August 12, 1949. https://ihl-databases.icrc.org/applic/ihl/ihl.nsf/INTRO/365. Accessed January 14, 2020.
- Protocol Additional to the Geneva Conventions of 12 August 1949, and relating to the Protection of Victims of International Armed Conflicts (Protocol 1). June 8, 1977. https://ihl-databases.icrc.org/applic/ihl/ihl.nsf/INTRO/470. Accessed January 14, 2020.
- Annas GJ. Military medical ethics – physician first, last, always. N Eng J Med. 2008;359(11):1087-1090.
- Lohman D. Retreat from human rights and adverse consequences for health. JAMA. 2018;319(9):861-862.
- Francis E. The war on Syria’s doctors. Foreign Policy. August 11, 2016. https://foreignpolicy.com/2016/08/11/the-war-on-syrias-doctors-assad-medicine-underground/. Accessed January 12, 2020.
- Lynch C. Across the Middle East, doctors are being killed like never before. Foreign Policy. March 2, 2016. https://foreignpolicy.com/2016/03/02/across-the-middle-east-doctors-are-being-killed-like-never-before/. Accessed January 12, 2020.
- U.S. Central Command. Summary of the Airstrike on the MSF Trauma Center in Kunduz, Afghanistan on October 3, 2015; Investigation and Follow-on Actions. April 29, 2016. https://www.centcom.mil/MEDIA/PRESS-RELEASES/Press-Release-View/Article/904574/april-29-centcom-releases-investigation-into-airstrike-on-doctors-without-borde/. Accessed January 15, 2020.
- Médecins Sans Frontières. Internal Review of the Kunduz Hospital Attack. November 5, 2015. https://www.msf.org/afghanistan-msf-releases-internal-review-kunduz-hospital-attack. Accessed January 14, 2020.
- Maurer P. War, protection and the law: the ICRC’s approach to international humanitarian law. May 19, 2014. https://www.ejiltalk.org/wp-content/uploads/2014/05/UK-2ndFCO-Int-Law-Lecture-Peter-Maurer-Final.pdf. Accessed January 15, 2020.
- International Committee of the Red Cross. Health Care in Danger. http://healthcareindanger.org/. Accessed January 12, 2020.
- United Nations Security Council. Resolution 2286. May 3, 2016. http://unscr.com/en/resolutions/doc/2286. Accessed January 14, 2020.
CHARLES G. KELS, Lt.Col, JD, is an attorney-adviser for the U.S. Department of State’s Bureau of Medical Services and a judge advocate (JAG) in the U.S. Air Force Reserve. He practices health and disability law and researches in the areas of medical privacy, informed consent, and professional ethics. The views expressed are those of the author alone and do not reflect those of the State Department, Air Force, or Department of Defense.
Submitted for the 2019–2020 Blood Writing Contest & Highlighted in Frontispiece Volume 12, Issue 2 – Spring 2020