Claire Elliott
London, Ukrain
Why do patients allow physicians to carry out an intimate examination barely ten minutes after they have met? As John Berger wrote in 1967, “We give the doctor access to our bodies. Apart from the doctor, we only grant such access voluntarily to lovers – and many are frightened to do even this.”1 Doctors need to be taught how to examine patients, and how to allow patients to give them permission to do so. The history of medicine helps us understand how this has come about and gain greater insight into the complexities involved. How did doctors negotiate the right to do this? How and why did patients allow it? How have doctors been trained to avoid crossing an unmarked boundary between clinical examination and something more intimate?
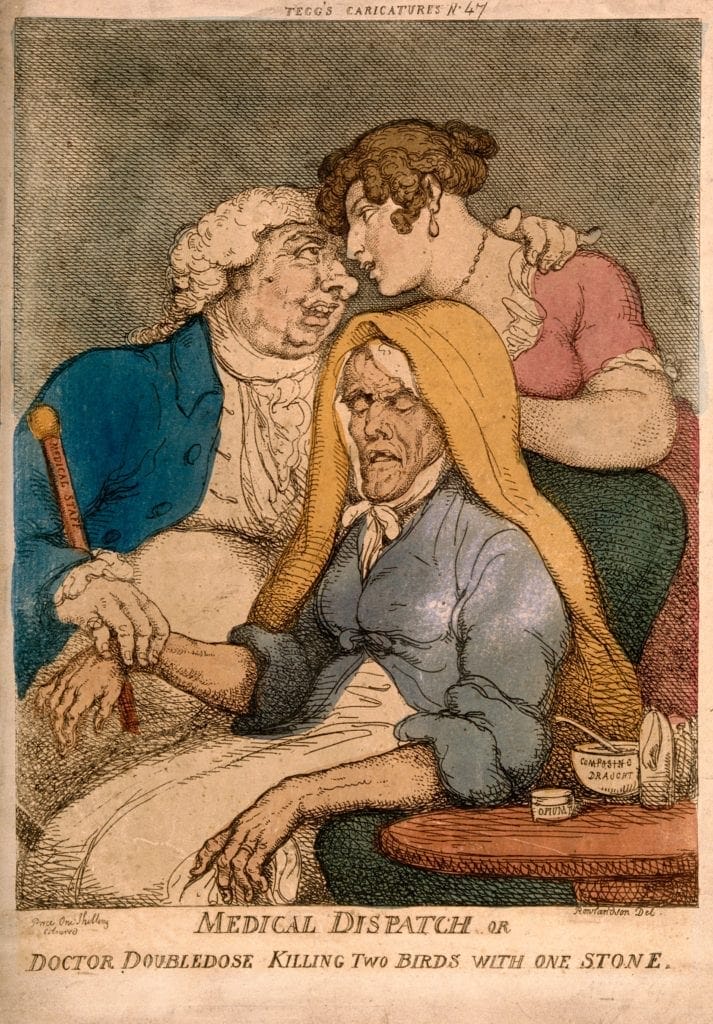
During the eighteenth century, there were many cartoons depicting doctors as sexual predators. In Thomas Rowlandson’s etching Medical Dispatch or Dr. Doubledose Killing Two Birds from 1810, a portly physician feels the pulse of a frail, elderly patient with one hand while squeezing the shoulder of the patient’s daughter (or maid) with the other, staring lasciviously into her eyes.2 The “Composing Draught” and the opium pillbox on the table suggest the physician may be deliberately sedating the patient to allow his libidinous ways to continue without interference. The physician’s implements such as the cane (labelled medical staff in Rowlandson’s cartoon), lancet, and syringe are motifs of sexual power and demand.
However, it is crucial to note that up to the eighteenth century, physical examination of patients was cursory and superficial. It might involve examination of the skin, taking the pulse, possibly checking the urine, looking at the tongue, and sniffing for bad odors. Chest, heart, and abdominal examination were not performed. History taking was key to the consultation and included detailed information about lifestyle, eating, sleeping, and bowel habits.
Changes in Western medicine during the nineteenth century allowed for closer examination of a patient’s body. The influence of Paris Medicine meant that patients were now rarely seen in their homes but instead were examined and treated in hospitals with medical students.3 Patients were grouped together by disease as specialities developed. With a shift away from humoral medicine and an infusion of science beginning in the late eighteenth century, the biomedical system developed. Doctors could now elicit physical signs of disease by examining the patient. Examination findings were later correlated with post mortem findings, and each doctor’s scientific knowledge and the patient’s subjective symptoms were now correlated with the physical examination. The doctor would inspect the patient’s body, palpate the abdomen, and listen to and percuss the chest (initially with one’s ear and later with a stethoscope).

As the medical profession developed into a more cohesive body bound by shared values, increased scientific knowledge, and a level of standardization of practice, physicians were allowed to penetrate more safely into the body of the patient. A doctor would hear about a symptom, then examine the patient to find the signs that would demonstrate the diagnosis. Foucault described this separation of body and personal identity as “the medical gaze.”
In the nineteenth century, patients were seen more often in hospitals, which helped establish the objective nature of disease. Patients started to be defined by their condition, as doctors focused on disease and specialties developed. This shift is described by Jewson as the “disappearance of the sick man.”4 Doctors no longer viewed patients as individuals but rather as a collection of signs that could only be found with special techniques on examination. A ritualized system of physical exam developed based on a biomedical understanding of body systems. This systematized way of examining a patient, beginning with inspection, followed by palpation and auscultation, allowed the physical exam to be viewed as clinical. However, by turning patients into a collection of signs to be discovered, a sense of the person as an individual was lost.
In the mid nineteenth century, national medical societies were established in most Western countries (British Medical Association in 1856, the American Medical Association or AMA in 1847). In the UK, the Medical Reform Act of 1858 resulted in the founding of the General Medical Council, which unified a single authority to grant medical licenses. This bound together the three branches of medicine—physicians, surgeons, and apothecaries—and of equal importance, excluded quacks, healers, and others. These medical societies promoted the interests and standards of their members and defended themselves against those not included. Society members were also bound by shared medical ethics such at the AMA Medical Ethics Code of 1847. Medical student education could now be controlled and monitored. It also helped patients to see doctors as a unified professional body that could be trusted.
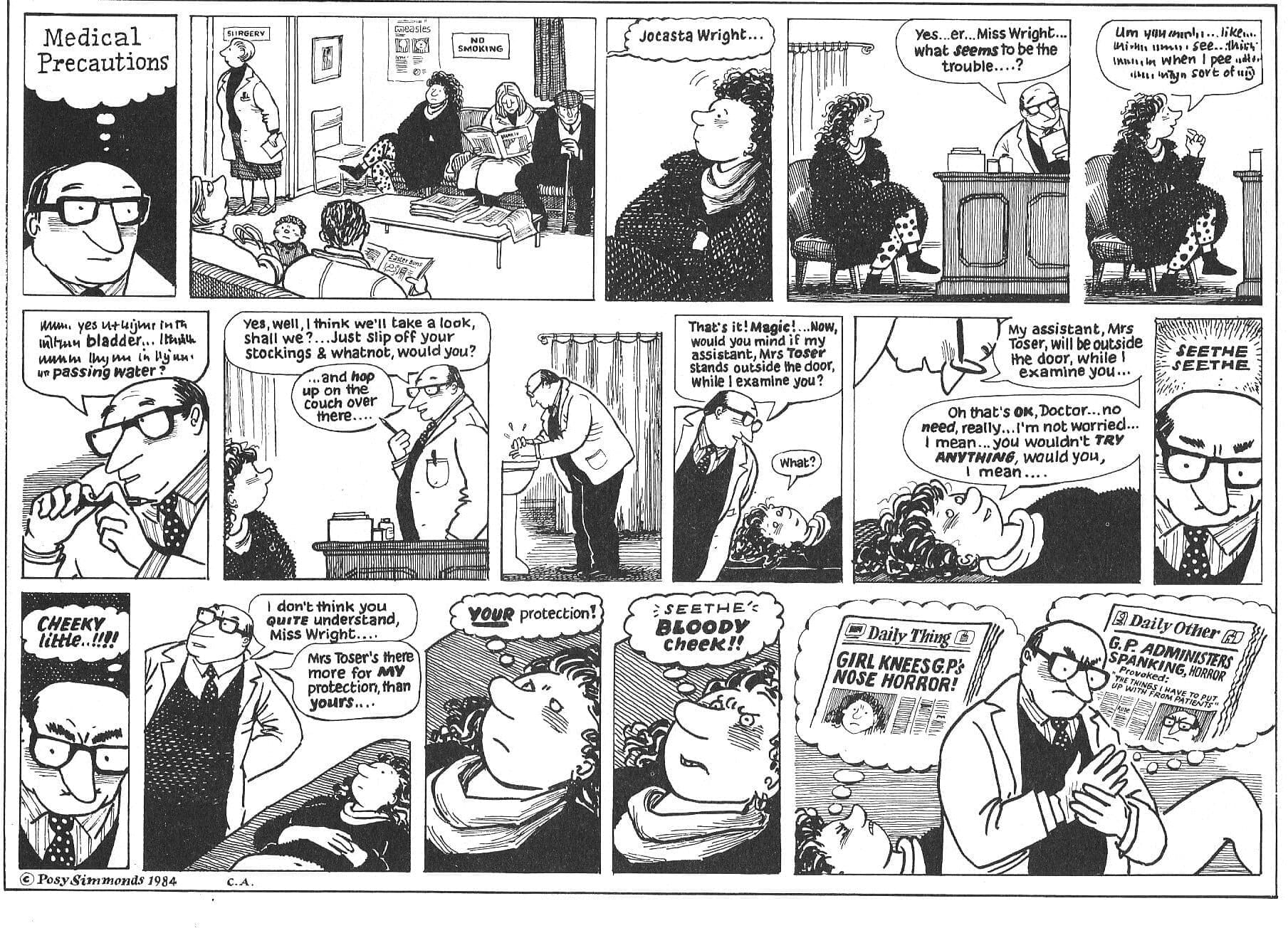
This history continues to have an impact on the practice of medicine today. Professional attire is seen as important to patient care, and professional organizations offer guidelines on how doctors should dress.5 Setting is also important, and the buildings of hospitals or outpatient settings are designed to be clinical areas with easy-to-clean floors and wall coverings in line with infection control guidance. Language should be factual and clear, avoiding the use of a personal pronoun to make it more objective (such as “I would like to carry out an internal examination”). There is a shared ethical code among doctors, which means that most doctors are trusted. Patients should be asked permission before examination and allowed to undress unobserved, then only exposing the relevant areas. Chaperones offer protection for both the patient and the doctor, as is shown in the Posy Simmonds cartoon.
Using the rituals of examination from the era of hospital medicine and having an order for examination, working through the body in a systematic way dictated by our understanding of anatomy and physiology, allows the patient to feel that the medical examination is based on clinical need and is confidential, consistent with the shared code of the profession. This allows patients to give consent for examination without suspicion. Working in a manner consistent with the professional changes developed over the past 200 years allows doctors to avoid being accused of the sexual impropriety—as was not uncommon in the eighteenth century.
References
- Berger John A Fortunate Man: The Story of a Country Doctor London Allen Lane Penguin Press, 1967
- Porter Roy Bodies Politic Disease, Death and Doctors in Britain, 1650-1900 (London: Reaktion Books 2001) 223-224
- Gelfand T Chap 47 The History of the Medical Profession in Bynum WF and Porter R Companion Encyclopaedia of the History of Medicine Vol 2 London Routledge 1127-1133
- Jewson N. The disappearance of the sick-man from medical cosmology, 1770–1870 Sociology 1976;10(2):225–244
- https://www.bma.org.uk/advice/employment/contracts/consultant-contracts/dress-code Accessed 13/3/19
CLAIRE ELLIOTT, MSc, MBBS, DFFP, DRCOG, MRCGP, is a general practitioner in Bloomsbury, London. She also teaches medical humanities at University College London Medical School and is responsible for developing and delivering courses for medical students and health professionals. Her interests include the history of medicine and literature and medicine. She has been the President for the History of Medicine Section at the Royal Society of Medicine and the book editor for the BMJ publication Medical Humanities.